


A REVIEW ON CANCER AND AN OVERVIEW OF METHOTREXATE DRUG
HTML Full TextA REVIEW ON CANCER AND AN OVERVIEW OF METHOTREXATE DRUG
Shristi Yadav * 1, Rohit Kumar Bijauliya 2, Dilip Kumar Chanchal 2 and Prashant Kumar Singh 3
Department of Pharmaceutics 1, Department of Pharmacognosy 2, Institute of Pharmacy, Bundelkhand University, Jhansi - 284128, Uttar Pradesh, India.
College of Pharmacy 3, Bareilly International University, Bareilly - 243006, Uttar Pradesh, India.
ABSTRACT: Cancer is a general term applied to a series of malignant diseases that may affect different parts of the body. Cancer is a disease which occurs when changes in a group of normal cells within the body lead to uncontrolled growth causing a lump called a tumor; this is true of all cancers except leukemia (cancer of the blood). When cancer spreads to other parts of the body, this is called metastasis. Methotrexate (MTX) is a folate antimetabolite used as an anticancer agent in the treatment of head and neck cancer, lung cancer, breast cancer. The doses and frequency of administration of MTX depend on its toxicity to hematopoietic tissues and buccal or gastrointestinal mucosa, drug resistance, leucopenia, and nephrotoxicity and limits its chemotherapeutic applications. Methotrexate is an antineoplastic antimetabolite. Anti-metabolites masquerade as purine or pyrimidine - which become the building blocks of DNA. They prevent these substances from becoming incorporated into DNA during the "S" phase (of the cell cycle), stopping normal development and division. Methotrexate is also indicated in the management of severe, active, classical, or definite rheumatoid arthritis. This review article is focused on cancer, its type, classification of anticancer drug and also discussed on pharmacokinetic and pharmacodynamics of methotrexate and its importance in the pharmacy field.
Keywords: Cancer, Methotrexate, Pharmacodynamics and Pharmacokinetics
INTRODUCTION: Cancer is a general term applied to a series of malignant diseases that may affect different parts of the body. These diseases are characterized by a rapid and uncontrolled formation of abnormal cells, which may mass together to form a growth or tumor or proliferate throughout the body, initiating abnormal growth at other sites.
If the process is not arrested, it may progress until it causes the death of the organism. The main forms of treatment for advanced stage cancer in humans are surgery, radiation, and drugs (cancer chemotherapeutic agents). Cancer chemotherapeutic agents can often provide temporary relief of symptoms, prolongation of life, and occasionally cures 1.
Many hundreds of chemical variants of a known class of cancer chemotherapeutic agents have been synthesized but have more side effects. A successful anticancer drug should kill or incapacitate cancer cells without causing excessive damage to normal cells.
This ideal is difficult, or perhaps impossible, to attain and is why cancer patients frequently suffer unpleasant side effects when undergoing treatment. Synthesis of modifications of the known drug continues as an important aspect of research. However, a waste amount of synthetic work has given relatively small improvements over the prototype drugs. There is a continued need for new prototype-new templates to use in the design of potential chemotherapeutic agents: natural products are providing such templates.
Recent studies of tumor-inhibiting compound of plant origin have yielded an impressive array of novel structures. Many of these structures are extremely complex, and it is most unlikely that such compounds would have been synthesized in empirical approaches to new drugs 2, 3. Cancer is a disease which occurs when changes in a group of normal cells within the body lead to uncontrolled growth causing a lump called a tumor; this is true of all cancers except leukemia (cancer of the blood). (Medical news today) When cancer spreads to other parts of the body, this is called metastasis 4.
Tumor: Benign tumors are not cancer. They usually can be removed and, in most cases, they do not come back. Most important, cells from benign tumors do not spread to other parts of the body. Cells from benign tumors stay together, and often they are surrounded by a containing membrane.
Malignant tumors are faster growing than benign tumors and can spread and destroy neighboring tissue. Cells of malignant tumors can break off from the main (primary) tumor and spread to other parts of the body through a process known as metastasis. Upon invading healthy tissue at the new site, they continue to divide and grow. These secondary sites are known as metastases, and the condition is referred to as metastatic cancer.
Cancer can be classified according to the following categories: 5
Carcinoma: cancer that arises from the epithelial cells (the lining of cells that helps protect or enclose organs). Carcinomas may invade the surrounding tissues and organs and metastasize to the lymph nodes and other areas of the body. The most common forms of cancer in this group are breast, prostate, lung, and colon cancer.
Sarcoma: A type of malignant tumor of the bone or soft tissue (fat, muscle, blood vessels, nerves, and other connective tissues that support and surround organs). The most common forms of sarcoma are leiomyosarcoma, liposarcoma, and osteosarcoma.
Lymphoma: Lymphoma is a cancer of the lymphatic system, which runs all through the body, and can, therefore, occur anywhere. The two main forms are non-Hodgkin's which begins with uncontrolled growth of the - white blood cells -lymphocytes - of the immune system) and Hodgkin's lymphoma in which cells of the lymph nodes become cancerous.
Leukemia: Leukaemia is a cancer of the white blood cells and bone marrow, the tissue that forms blood cells. There are several subtypes; common are lymphocytic leukemia and chronic lymphocytic leukemia.
Signs and Symptoms: 6 As there are so many different types of cancer, the symptoms are varied and depend on where the disease is located. However, there are some key signs and symptoms, including:
Lumps: Some cancers can be felt through the skin. Cancerous lumps are often painless and may increase in size as cancer progresses.
Coughing, Breathlessness: Persistent coughing episodes and breathlessness can be associated with lung cancer.
Changes in Bowel Habits: Symptoms of bowel cancer may include blood in the stools and a change in bowel habits such as constipation and diarrhea.
Bleeding: Any unexpected bleeding can be a sign of cancer:
- Bleeding from the anal passage may be a sign of bowel cancer.
- Bleeding from the cervix may be a sign of cervical cancer.
- Blood present in the urine may be a sign of kidney or bladder cancer.
Unexplained Weight Loss: A large amount of unexplained weight loss over a short period (a couple of months) can be a sign of cancer.
Fatigue: Fatigue is extreme tiredness and a severe lack of energy. If fatigue is due to cancer, sufferers normally also have other symptoms.
Treatment for Cancer: The treatment given for cancer is variable and dependent on several factors, including the type, location, and amount of disease and the health status of the patient. Most treatments are designed to either directly kill/remove the cancer cells or to lead to their eventual death by depriving them of signals needed for cell division. Other treatments work by stimulating the body's own defense against the cancer cells. The good news is that about half of all cancers diagnosed are now curable. Even with cancers that cannot be cured, symptoms are often greatly diminished by treatment. Treatment options, which depend on the stage and type of cancer, include:
- Surgery
- Radiation therapy
- Chemotherapy
- Biological therapy
- Hormone therapy
1. Surgery: Surgery about 60% of people with cancer have some sort of surgery. If the tumor is in one place and can be removed without interfering with body functions, then surgery may be the best approach.
2. Radiation Therapy: Radiation therapy is done to shrink tumors or to make them disappear. This can be done by directing beams of X-rays or other high-energy rays at the tumor site. Radioactive materials can also be placed in or near the tumor.
3. Chemotherapy Radiation: Chemotherapy radiation and surgery are often used to treat cancer that is in one part of the body. Chemotherapy may be used to treat cancer that has spread. Treatment can also be a combination of surgery, radiation, and chemotherapy. Some chemotherapy chemicals can be taken by mouth; others need to be taken intravenously (into the blood through a vein). Chemotherapy can sometimes cause unpleasant side effects.
4. Biological Therapy: Biological therapy uses treatments that help the immune system do its job of fighting disease in our bodies. This can be an effective treatment for some cancers.
5. Hormone Therapy: For cancers that need hormones to grow, hormonal therapy can be an option. With this therapy, the production of hormones is reduced through surgery or medication
Antibodies: Antibodies are naturally occurring proteins in our bodies, which act by either depriving the cancer cells of necessary signals or causing the direct death of the cells.
Vaccines: Vaccines usually contain proteins found on or produced by cancer cells when administered these proteins increase the response of the body against the cancer cells 6, 7.
Causes of Cancer: Modern medicine attributes most cases of cancer to changes in DNA that reduce or eliminate the normal controls over cellular growth, maturation, and programmed cell death. These changes are more likely to occur in people with certain genetic backgrounds (as illustrated by the finding of genes associated with some cases of cancer and familial prevalence of certain cancers) and in persons infected by chronic viruses (e.g., viral hepatitis may lead to liver cancer; HIV may lead to lymphoma). The ultimate cause, regardless of genetic propensity or viruses that may influence the risk of the cancer, is often exposure to carcinogenic chemicals (including those found in nature) and / or to radiation (including natural cosmic and earthly radiation), coupled with a failure of the immune system to eliminate the cancer cells at an early stage in their multiplication. The immunological weakness might arise years after the exposure to chemicals or radiation. Other factors such as tobacco smoking, alcohol consumption, excess use of caffeine and other drugs, sunshine, infections from such oncogenic virus, like cervical papillomaviruses, adenoviruses Kaposi's sarcoma (HSV) or exposure to asbestos. These are implicated as causal agents of mammalian cancers.
However, a large population of people is often exposed to these agents. Consequently, cancer cells continue to divide even in situations in which normal cells will usually wait for a special chemical transduction signal. The tumor cells would ignore such stop signals that are sent out by adjacent tissues. A Cancer cell also has the character of immortality even in-vitro, whereas normal cells stop dividing after 50-70 generations and undergo programmed cell death (Apoptosis). Cancer cells continue to grow to invade nearby tissues and metastasize to distant parts of the body. Metastasis is the most lethal aspect of carcinogenesis 8.
Environmental factors which, from a scientist’s standpoint, include smoking, diet, and infectious diseases as well as chemicals and radiation in our homes and workplace along with trace levels of pollutants in food, drinking water and in air. Other factors which are more likely to affect are tobacco use, unhealthy diet, not enough physical activity; however, the degree of risk from pollutants depends on the concentration, intensity, and exposure. The cancer risk becomes highly increased where workers are exposed to ionizing radiation, carcinomas chemicals, certain metals, and some other specific substances even exposed at low levels. Passive tobacco smoke manifold increases the risk in a large population who do not smoke but exposed to exhaled smoke of smokers 9.
The Mechanism on Cancer Therapy: 10
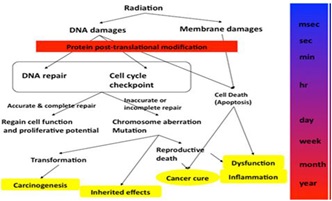
FIG. 1: THE MECHANISM ON CANCER THERAPY
- Inhibiting cancer cell proliferation directly by stimulating macrophage phagocytosis, enhancing natural killer cell activity.
- Promoting apoptosis of cancer cells by increasing production of interferon, interleukin-2 immunoglobulin, and complement in blood serum.
- Enforcing the necrosis of the tumor and inhibiting its translocation and spread by blocking the blood source of tumor tissue.
- Enhancing the number of leukocytes and platelets by stimulating the hemopoietic function.
- Promoting the reverse transformation from tumor cells into normal cells.
- Promoting metabolism and preventing carcinogenesis of normal cells.
- Stimulating appetite, improving quality of sleep, relieving pain, thus benefiting patient’s health.
Oncogenes and Tumor Suppressor Genes: Two sets of genes are controlling cancer development 11. Oncogenes are the first set of genes and are involved in different cell activities, including cell division. However, overexpression of these genes transforms a normal cell into a cancer cell. On the other hand, the second set of genes (tumor suppressor genes) inhibits cancer cell formation by different mechanisms.
Tumor suppressor genes are underexpressed in cancer cells, while oncogenes are overexpressed 12. Summarizes the main oncogenes and tumor suppressor genes and their role in cancer development. Oncogenes and their products represent good targets for Cancer therapy. Other targets include enzymes involved in cell division like topoisomerases that unwind the DNA during replication. The diversity of plant-derived natural products can provide therapeutic products attacking different targets in cancer cells 13.
Cellular Kinetics:
Cell Cycle: Uncontrolled cell division is a result of interference in the normal balance of the cell cycle. The cell cycle is divided into several phases governed by an elaborate set of molecular switches. Normal nondividing cells are in G0. When actively recruited into the cell cycle, they then pass through four phases:
G1: the growth phase in which the cell increases in size and prepares to copy its DNA;
S (Synthesis): which allows doubling of the chromosomal material, i.e. the cell copies its DNA to make 2 sets of chromosomes - one set for each new cell
G2: a further growth phase before cell division i.e. the cell makes more proteins in preparation for cell division.
M (Mitosis): where the chromosomes separate, and the cell divides.
At the end of a cycle, the daughter cells can either continue through the cycle or leave and enter the resting phase (G0) or become terminally differentiated.
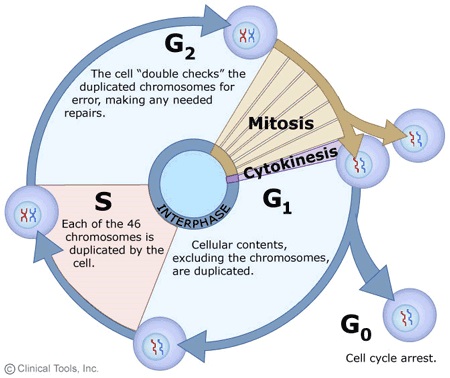
FIG. 2: CELL CYCLE
Classification of Anticancer Drugs: 14
- Polyfunctional Alkylating Agents:
- Nitrosoureas
- Mustards (Nitrogen Mustards)
- Methanesulphonates (Busulphan)
- Ethylenimines
- Other Alkylating Drugs:
- Procarbazine (Matulane)
- Dacarbazine (DTIC)
- Altretamine (Hexalen)
- Cisplatin (Platinol)
- Antimetabolites:
- Antifolic acid compounds (Methotrexate)
- Amino acid Antagonists (Azaserine)
- Purine Antagonists:
- Mercaptopurine (6-MP)
- Thioguanine (6-TG)
- Fludarabine Phosphate
- Cladribine (Leustatin)
- Pentostatin (Nipent)
- Pyrimidine Antagonists:
- Fluorouracil (5-FU)
- Cytarabine (ARA-C)
- Azacitidine
- Plant Alkaloids:
- Vinblastine (Velban)
- Vincristine (Oncovin)
- Etoposide (VP-16,VePe-sid)
- Teniposide (Vumon)
- Topotecan (Hycamtin)
- Irinotecan (Camptosar)
- Paclitaxel (Taxol)
- Docetaxel (Taxotere)
- Antibiotics:
- Anthracyclines
- Doxorubicin (Adriamycin, Rubex, Doxil)
- Daunorubicin (DaunoXome)
- Dactinomycin (Cosmegen)
- Idarubicin (Idamycin)
- Plicamycin (Mithramycin)
- Mitomycin (Mutamycin)
- Bleomycin (Blenoxane)
- Monoclonal Antibodies:
- Hormonal Agents:
- Tamoxifen (Nolvadex)
- Flutamide (Eulexin)
- Gonadotropin-Releasing Hormone Agonists
- (Leuprolide and Goserelin (Zoladex))
- Aromatase Inhibitors
- Aminoglutethimide
- Anastrozole (Arimidex)
- Miscellaneous Anticancer Drugs:
- Amsacrine
- Hydroxyurea (Hydrea)
- Asparaginase (El-spar)
- Mitoxantrone (Novantrone)
- Mitotane
- Retinoic acid derivatives
- Bone marrow growth factors
- Amifostine
Methotrexate: Methotrexate (MTX) is a folate antimetabolite used as an anticancer agent in the treatment of head and neck cancer, lung cancer, breast cancer 15. The doses and frequency of administration of MTX depend on its toxicity to hematopoietic tissues and buccal or gastrointestinal mucosa, drug resistance, leucopenia and nephrotoxicity and limits its chemotherapeutic applications 16, 17.
There are many attempts have been made to reduce the adverse effect and improve both the specificity and selective of MTX. For instance, controlled release of anti-neoplastic agents is of real interest as it keeps a low level of circulating concentrations, therefore avoiding iatrogenic secondary effects. Also, it particularly increased the efficiency of MTX and similar chemotherapeutic agent, which requires long-term administration of small doses of the drug for effective cancer management 17.
Methotrexate is used to treat certain types of cancer or to control severe psoriasis or rheumatoid arthritis that has not responded to other treatments. It may also be used to control juvenile rheumatoid arthritis. Methotrexate belongs to a class of drugs known as antimetabolites. It works by slowing or stopping the growth of cancer cells and suppressing the immune system. Early treatment of rheumatoid arthritis with more aggressive therapy such as methotrexate helps to reduce further joint damage and to preserve joint function. There is a lack of clear clinical recommendation / universally accepted regimens for the use of MTX in patients because of the variability and unpredictability of the pharmacological action with relatively high toxicity. Therefore the variability regarding MTX starting dosage, dosage increment size, the interval between increments, and the route of administration 16.
TABLE 1: DESCRIPTION OF METHOTREXATE
| Molecular Wt. | 454.44 g/mol |
| Molecular formula | C20H22N8O5 |
| Dose | 15 to 30 mg daily |
| Solubility | Soluble in alkali hydroxide and carbonates |
| Routes of administration | Oral, IV, IM, SC, Intrathecal |

FIG. 3: STRUCTURE OF METHOTREXATE
TABLE 2: PHARMACOKINETICS
| Bioavailability | 60% at a lower dose,
Less at higher dose |
| Protein binding | 35-50% (parent drug) |
| Metabolism | Hepatic and Intracellular |
| Half-Life | 3-10 hrs (lower dose)
8-15 hrs (higher dose) |
| Excretion | Urine (80-100%)
Faces (small amount) |
Pharmacodynamics: Methotrexate is an antineoplastic antimetabolite. Anti-metabolites masquerade as purine or pyrimidine - which become the building blocks of DNA. They prevent these substances from becoming incorporated into DNA during the "S" phase (of the cell cycle), stopping normal development and division. Methotrexate inhibits folic acid reductase which is responsible for the conversion of folic acid to tetrahydrofolic acid. At two stages in the biosynthesis of purine and one stage in the synthesis of pyrimidine, one-carbon transfer reactions occur which require specific coenzymes synthesized in the cell from tetrahydrofolic acid.
Tetrahydrofolic acid itself is synthesized in the cell from folic acid with the help of an enzyme, folic acid reductase. Methotrexate looks a lot like folic acid to the enzyme, so it binds to it quite strongly and inhibits the enzyme. Thus, DNA synthesis cannot proceed because the coenzymes needed for one-carbon transfer reactions are not produced from tetrahydrofolic acid because there is no tetrahydrofolic acid. Methotrexate selectively affects the most rapidly dividing cells (neoplastic and psoriatic cells). Methotrexate is also indicated in the management of severe, active, classical, or definite rheumatoid arthritis
Mechanism of Action: Methotrexate mechanisms of action are only partially known and understood. MTX is an antimetabolite and a folate analog with only minor structural differences, designed to compete for folate receptors. It enters cells through an active transport mechanism and by facilitated diffusion, and once inside the cell, it is converted into polyglutamated MTX by folylpolyglutamyl synthase. Polyglutamated MTX reversibly inhibits dihydrofolate reductase but also inhibits other enzymes, especially thymidylate synthase and 5-aminoimidazole- 4 -carboxamide ribonucleotide (AICAR) transformylase.
Reduced folate (tetrahydrofolate [THF]) is involved in the de novo synthesis of purine and pyrimidine precursors of DNA and RNA. THF is also important for the methylation of DNA, RNA, and other proteins, such as homocysteine. Ultimately, MTX is eliminated from the cell by transporters of the ATP-binding cassette family. Methotrexate can inhibit proliferation and induce apoptosis of neoplastic cells and was therefore first used at the end of the 1940s by hematologists. Indeed, MTX also possesses a variety of anti-inflammatory effects at low doses, that is, those prescribed by rheumatologists. MTX inhibits T-cell activation and proliferation, downregulates the expression of some activation and adhesion molecules, for example, intercellular adhesion molecule-1 decreases immunoglobulin production, inhibits cyclooxygenases and lipooxygenases, and modulates monocyte and macrophage secretion of various cytokines.
Most of these anti-inflammatory effects probably reflect the inhibition of AICAR transformylase, causing the accumulation of AICAR, and thus enhancing adenosine release into the blood. Extracellular adenosine can bind to trans-membrane-spanning adenosine surface receptors, especially types A2a and A3, resulting in the subsequent inhibition of phagocytosis, lymphocyte proliferation, and altered synthesis and secretion of several proinflammatory cytokines, such as TNF-α, IL-12, and IFN-γ.
Indication: Methotrexate plays an important role in the chemotherapy of malignant tumors despite its considerable side-effects. Women with choriocarcinoma and other trophoblastic tumors can often be cured with the sole use of methotrexate. Methotrexate is also the drug of choice for the maintenance therapy of acute lymphocytic leukemia (after remission has been induced with other drugs). An intrathecal application of methotrexate also lowers the risk of leukemic meningeal involvement.
Methotrexate is combined with other cytostatics for the treatment of many other tumors. Important examples are non-Hodgkin's lymphoma, breast carcinoma, small-cell lung carcinoma, epidermal tumors on the head and neck, and ovarian carcinoma. High doses of methotrexate are administered for osteosarcoma (in combination with calcium folate). Small oral doses of methotrexate are effective against severe forms of chronic polyarthritis and psoriasis. Only subjects for whom other therapies were ineffective or who experienced severe side-effects may be treated with methotrexate. In 90% of cases, methotrexate can help avoid surgical intervention for an extrauterine pregnancy. Methotrexate has similar effects as cyclosporine for graft-versus-host disease.
Absorption: Oral absorption is dose dependent on adults and leukemic pediatric patients. In adults, peak serum levels are reached within one to two hours. At doses of 30 mg/m2 or less, methotrexate is generally well absorbed with a mean bioavailability of 60%. At doses greater than 80 mg/m2, the absorption of the doses is significantly less due to a saturation effect.
The volume of Distribution:
- 18 L/kg [initial volume of distribution (Vd)]
- 4 - 0.8 L/kg [steady state Vd] Methotrexate competes with reduced folates for active transport across cell membranes using a single carrier-mediated active transport process. At serum concentrations greater than 100 micro molars, passive diffusion becomes a major pathway by which effective intracellular concentrations can be achieved. Methotrexate does not cross the blood-brain-barrier.
Metabolism: After adsorption MTX undergoes hepatic and intracellular metabolism to polyglutamated forms which can be converted back to MTX by hydrolase enzyme. These polyglutamates act as inhibitors of dihydrogenfolate reductase and thymidylate synthetase. A small amount of MTX polyglutamate may remain in tissues for an extended period. The retention and prolonged drug action of these active metabolites vary among different cells, tissue, and tumors. A small amount of metabolism to 7-hydroxymethotrexate may occur at doses commonly prescribed.
Route of Elimination: Renal excretion is the primary route of elimination and is dependent upon dosage and route of administration. IV administration, 80% to 90% of the administered dose is excreted unchanged in the urine within 24 hours. There is limited biliary excretion amounting to 10% or less of the administered dose.
Drug Interaction: Penicillin may decrease the elimination of methotrexate, so increase the risk of toxicity. The aminoglycosides neomycin and paromomycin, have been found to reduce gastrointestinal (GI) absorption of methotrexate. Probenecid inhibits methotrexate excretion, which increases the risk of methotrexate toxicity.
Adverse Reactions: The most important and the most dangerous are bone marrow depression (leucopenia, thrombocytopenia, anemia) and gastrointestinal mucositis (stomatitis, diarrhea). Liver damages are also frequent (an acute increase of the transaminases, cirrhosis of the liver in 10% or more after chronic oral therapy). The doses used in chemotherapy cause nausea and vomiting in 20% of the treated subjects. Various skin reactions, asthma, pneumonitis, and vacuities are possible. Nephrotoxic effects are to be expected mainly after high doses. There are neurological complications (arachnoiditis, rigidity, late encephalopathy) after intrathecal application or high dosage.
For its rheumatologic indications, MTX is usually administered at a weekly dose of 0.2-0.3 mg/kg, for example, 10-25 mg/week, most frequently administered orally, or injected intramuscularly or subcutaneously. For inflammatory myopathies, higher doses of up to 40 mg/week are generally prescribed. Regardless of the route and dose, its bioavailability is good, reaching 90% when given subcutaneously and up to 75% when taken orally, but it may be more variable with oral doses over 25 mg/week. MTX is eliminated through the kidneys with nonlinear kinetics due to its tubular secretion-reabsorption cycle, which can be altered in renal insufficiency or certain conditions, such as with the co-prescription of high-dose aspirin, thereby potentially increasing its toxicity. Notably, the dose administered more closely parallels its toxicity than its efficacy, and adverse events can occur before the expected therapeutic benefit of MTX. Indeed, there is a latent period of several weeks before the MTX efficacy in patients can be appreciated and evaluated.
Adverse events are the main factor influencing the decision to discontinue MTX; they can be minor, for example, gastrointestinal intolerance (occurs in up to 70% of the patients), or more severe, like pancytopenia (occurs in 0.9-1.4% or liver cirrhosis (occurs in 0-2%). Indeed, 10-37% of patients terminate MTX treatment owing to an adverse event. Potential and more important adverse events of MTX to keep in mind, along with its contraindications. Some MTX adverse events are due to folate antagonism and closely resemble those seen in patients with folate deficiency, such as elevated erythrocyte mean corpuscular volume or folate-deficiency anemia. Thus, folate supplementation allowed 83% of patients with rheumatoid arthritis to continue MTX at 48 weeks in the study by van Ede et al., compared with 62% of those receiving MTX without supplementation (p<0.001, with either folic or folinic acid).
However, while there is a basis for using folate supplementation to reduce adverse effects, the results of some studies suggested that adding folic acid to MTX could lead to a small loss of efficacy, due to their competition and interferences. However, the meta-analysis by Ortiz et al. did not demonstrate the consistent influence of such folate supplementation on disease activity. No consensus exists regarding the dose and frequency of folate supplementation. In any case, it seems important to delay folate supplementation for 48 h after MTX administration, because the timing of the folic or folinic acid intake about MTX might, at least in part, influence MTX efficacy.
Baseline and serial complete blood counts, and determination of keratinizing level, aspartate aminotransferase, alanine aminotransferase, and albumin are recommended every 2-4 weeks for the first 3 months of therapy and after each dose increment, then every 8-12 weeks for the 3 following months, and every 12 weeks after that. Older patients and those with alcohol dependence, multiple underlying diseases or comorbidities, especially chronic hepatitis or renal impairment, should be monitored more closely if MTX is not already contraindicated.
Dosage of serum MTX levels lack reliability for predicting adverse events, and that of its intracellular polyglutamate metabolites is technically difficult and not widely available. Methylene THF reductase (MTHFR) is not directly inhibited but is influenced by MTX effects on the intracellular folate pool. The presence of either the heterozygous or homozygous C677T mutation in the MTHFR gene leads to further homocysteine accumulation and is associated with increased risk of elevated transaminases, hair loss or gastrointestinal symptoms during MTX treatment, and ultimately, the necessity to stop MTX. The homozygous or heterozygote C677T variants have a respective prevalence of 8-10% and 40% in the general population. Conversely, the C allele of the A1298C polymorphism was found to be associated with better efficacy in rheumatoid arthritis, at least when compared with another 1298A/A homozygous genotype.
However, because the determination of MTHFR genotype is not yet widely available in every clinical facility, and because MTX metabolism seems to be influenced by many gene products, cost-effectiveness studies have to demonstrate the advantages of MTX pharmacogenetic assays over simple patient follow-up with serial monitoring 18.
CONCLUSION: Cancer is a general term applied to a series of malignant diseases that may affect different parts of the body. Cancer is a disease which occurs when changes in a group of normal cells within the body lead to uncontrolled growth causing a lump called a tumor; this is true of all cancers except leukemia (cancer of the blood). Methotrexate (MTX) is a folate antimetabolite used as an anticancer agent in the treatment of head and neck cancer, lung cancer, breast cancer. This review article is show suitable information of cancer and methotrexate drug.
ACKNOWLEDGEMENT: The authors thanks to the authorities of Institute of Pharmacy, Bundelkhand University, Jhansi, Uttar Pradesh for providing all the support to study and all other necessary facilities like internet surfing, library and other technical support to write the review article.
CONFLICT OF INTEREST: Nil
REFERENCES:
- Bhutani KK and Gohil VM: Natural product drug discovery research in India: Status and appraisal. Ind J Exp Bio 2010; 48: 199-207.
- Tyler V: Herbs of choice. The therapeutic use of phytomedicinals. New York: Haworth Press 1994; 24-26.
- Bijauliya RK, Alok S, Singh M and Mishra SB: A comprehensive review on cancer and anticancer herbal drugs. Int J Pharm Sci Res 2017; 8(7): 2740-61. doi: 10.13040/IJPSR.0975-8232.8(7).2740-61.
- National Cancer Institute. Available from: http:// www.cancer.gov.
- Cancer Reaserch UK. Available from: http:// cancer help.cancerresearchuk.org/.
- Macmillan Cancer Support. Available from http:// www.macmillan.org.uk/Cancerinformation.
- https://en.wikipedia.org/wiki/American_Cancer_Society
- McNutt K: Medicinals in foods. Nutr Today 1995; 30: 218-22.
- Krishnamurthi K: Screening of natural products for anticancer and antidiabetic properties. Health Administrator 2000; 20(1-2): 69.
- Cancer web site. Available at: http/www.cancer.gov.
- Wamidh HT: Anticancer and antimicrobial potential of plant-derived natural products, phytochemicals. Bio-activities and Impact on Health 2011; 142-158.
- Ghosh A, Das B, Roy A, Mandal B and Chandra G: Antibacterial activity of some medicinal plant extracts. Journal of Natural Medicines 2008; 62: 259-262.
- Grayer R and Harborne J: A survey of antifungal compounds from plants. Phytochemistry 1994; 37: 19-42.
- http://www.pharmatips.in/Articles/Pharmacology/Classification-of-Anticancer-Drugs.aspx
- Snyder RD: Some aspects of the development of metho-trexate therapy. Clin Exp Pharmacol Physiol Suppl 1979; 5:1-4.
- Chanbner BA, Allegra CJ, Curt JA and Calabresi P:. Antineoplastic agents. In: Hardman JG, Limbird LE, Molinoff PB, Ruddon RW, Gilman AG, ed. Goodman and Gilman’s pharmacological basis of therapeutics. New York: Mc Graw-Hill, 1996; 1243-1247.
- Lebugle A, Rodrigues A, Bonnevialle P, Voigt JJ, Canal P and Rodriguez F: Study of implantable calcium phosphate systems for the slow release of methotrexate. Biomaterials 2002; 23:3517-3522.
- https://www.drugbank.ca/drugs/DB00563
How to cite this article:
Yadav S, Bijauliya RK, Chanchal DK and Singh PK: A review on cancer and an overview of methotrexate drug. Int J Life Sci & Rev 2018; 4(10): 163-71. doi: 10.13040/IJPSR.0975-8232.IJLSR.4(10).163-71.
All © 2015 are reserved by International Journal of Life Sciences and Review. This Journal licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 3.0 Unported License.
Article Information
2
163-171
664
1412
English
IJLSR
S. Yadav *, R. K. Bijauliya, D. K. Chanchal and P. K. Singh
Department of Pharmaceutics, Institute of Pharmacy, Bundelkhand University, Jhansi, Uttar Pradesh, India.
simrenyadav90@gmail.com
10 August 2018
24 September 2018
30 September 2018
10.13040/IJPSR.0975-8232.IJLSR.4(10).163-71
01 October 2018