


A REVIEW ON PEDICULUS HUMANUS CAPITIS BASED ON LIFE CYCLE, RESISTANCE, SAFETY CONSIDERATIONS AND TREATMENT
HTML Full TextA REVIEW ON PEDICULUS HUMANUS CAPITIS BASED ON LIFE CYCLE, RESISTANCE, SAFETY CONSIDERATIONS AND TREATMENT
Shankar N. Bharti *, Milind J. Umekar and Nandkishor J. Duragkar
Smt. Kishoritai Bhoyar College of Pharmacy, New Kamptee, Nagpur - 441002, Maharashtra, India.
ABSTRACT: Head lice infestation or Pediculosis capitis, caused by Pediculus humanus capitis, is a common health concern. In the US, where Pediculosis capitis is the most prevalent parasitic infestation of children, 6 to 12 million people are affected every year. Pediculosis capitis remains confined to the scalp. Scalp pruritus is the cardinal symptom, although patients with lice can be asymptomatic. Pruritus with impetiginization should prompt the physician to look for lice or viable nits. All close contacts should be examined. Treatment directed at killing the lice and the ova should be considered only if active lice or viable eggs are observed. The three fundamental effective treatment options for head lice are topical pediculicides, wet combing, and oral therapy. Spraying or fogging a home with insecticides or pediculicides is not recommended.
Keywords: Pediculus capitis, The life cycle of head lice, Transmission, Symptoms, Treatment
INTRODUCTION: Pediculosis capitis, also known as head lice infestation, caused by Pediculus humanus capitis, is a frequent community health concern 1. Infestation occurs most commonly in children, with a peak incidence between 5 and 13 years of age. Although P. humanuscapitis is not a vector of human disease and poses no significant health risk to infested persons, head lice infestation can cause substantial social distress, discomfort, parental anxiety, an embarrassment to the child, and unnecessary absence from school and work. Lice egg sheaths, referred to as nits, are firmly glued to individual hairs. Eggs are 0.8 mm in length and are laid within 1 to 2 mm of the scalp surface.
Rarely, nits can be seen along the length of the hair shaft. One female can lay about 150 eggs during a 30-day life span. Young lice hatch within 1 week and go through 3 nymphal instar stages, growing larger and maturing to adults over 7 days 2-4.

FIG. 1: HEAD LICE INFESTATION, OR PEDICULOSIS CAPITIS
The first and second instar forms are relatively immobile and therefore are not easily transmitted between individuals; the most spread is related to the third instar forms and adults. Head lice can survive for up to 3 days off the host; nits can endure 10 days of separation from the host 5.
Characteristics of Lice: The head louse, Pediculus humanus capitis, is a host-specific arthropod that is 1 to 3 mm long and is grayish-whitish in color. It has narrow sucking mouthparts concealed within the head, short antennae, and three pairs of clawed legs adapted for grasping the hair. A louse feeds by sucking blood and simultaneously injecting saliva with vasodilatory and anticoagulation properties into the host. Head lice move at a speed of up to 23 cm/min and are incapable of jumping or flying. Lice egg sheaths, referred to as nits, are firmly glued to individual hairs. Eggs are 0.8 mm in length and are laid within 1 to 2 mm of the scalp surface. Rarely, nits can be seen along the length of the hair shaft.
One female can lay about 150 eggs during a 30-day life span. Young lice hatch within 1 week and go through 3 nymphal instar stages, growing larger and maturing to adults over 7 days. The first and second instar forms are relatively immobile and therefore are not easily transmitted between individuals; the most spread is related to the third instar forms and adults. Head lice can survive for up to 3 days off the host; nits can endure 10 days of separation from the host 6-8. New bites may cause reactivation of already healed bites. The most likely cause of the bite reactions seems to be the inflammatory response to injected louse saliva or anticoagulant. At the time of the first lice infestation, pruritus may not be seen for 1 to 2 months because it takes time to develop sensitivity. Therefore, by the time the patient is symptomatic, he or she may have been infested for at least 1 month already.
Epidermiologic Characteristics: Pediculosis capitis affects about 6 to 12 million people every year. The prevalence of head lice remains high. No age or economic stratum is immune to P. humanus capitis, although crowded living conditions tend to be associated with a higher prevalence of infestation. P. humanus capitis is the most common parasitic infection of children. Head lice infestation is not influenced by hair length or frequency of shampooing or brushing. Girls are about twice as likely to get head lice as boys. Infestations in the US are less common in blacks, due to physical characteristics of their hair shaft, which is more oval-shaped and is, therefore, more difficult to grasp.
Head-to-head contact is the most important mode of transmission. Pediculosis capitis can be transmitted by infested clothing, hats, hairbrushes, combs, towels, bedding, and upholstery 9.
Clinical Manifestations: Head lice infestations are characterized by nits attached to hairs approximately 0.7 cm from the scalp. Nits are often found in the occipital and retro-auricular portions of the head and are easier to observe than crawling adult lice. Pruritus is the principal symptom, although patients with lice can be asymptomatic. Bite reactions, excoriations, secondary impetigini-zation, pyoderma, cervical lymphadenopathy, conjunctivitis, fever, and malaise are also possible manifestations. Pyoderma may be accompanied by alopecia. A morbilliform hypersensitivity rash can mimic a viral exanthema. In longstanding cases, dermatitis of variable severity can be seen, characterized by exudation and crusting, especially in the occipital region. Uncommonly, in heavily infested and untreated patients, the hair can become tangled with exudates, predisposing the area to fungal infection. This results in a malodorous mass. Countless lice and nits can be found under the entangled hair mass 10. New bites may cause reactivation of already healed bites. The most likely cause of the bite reactions seems to be the inflammatory response to injected louse saliva or anticoagulant 11. At the time of the first lice infestation, pruritus may not be seen for 1 to 2 months because it takes time to develop sensitivity. Therefore, by the time the patient is symptomatic, he or she may have been infested for at least 1 month already.
Histopathologic Characteristics: The classic lesion shows a deep wedge-shaped intradermal hemorrhage with a perivascular infiltrate of lymphocytes, histiocytes, and eosinophils within the dermis 12.
Diagnosis: The gold standard for diagnosing head lice is the identification of a live louse, nymph, or a viable nit on the head. Because head lice avoid light and crawl quickly, visual inspection without combing is difficult 13. Using lice combs increases the chances of finding live lice and is a helpful screening tool. The diagnosis of lice infestation using a lice comb is fourfold more efficient than a direct visual examination. The tiny nits are easier to observe, especially at the nape of the neck or behind the ears. Nits by themselves are not diagnostic of an active infestation. However, if the nits are found within 0.7 cm of the scalp, an active infestation is likely. Recognition can be facilitated by a magnifying glass. Wood’s lamp examination reveals yellow-green fluorescence of the lice and their nits. Dermoscopy is also a possible aid in the diagnosis and follow-up of pediculosis capitis. There are new generations of handheld dermoscopes that do not require direct contact, preventing the possible risk of transferal. Pruritus with impetiginization should alert the physician to look for lice or viable nits 14.
Dead eggs can remain glued to the hair shafts for as long as 6 months. Human hair grows at a rate of approximately 1cm/month. As the hair grows, the cemented empty nits move away from the scalp. After 2 to 3 months, these empty nits become more visible, especially on dark hair. This appearance of “nits” several months after treatment can lead to a false-positive diagnosis of an active infestation because most people cannot differentiate between viable and empty eggs, and assume that if eggs are present, the child must also have lice. Therefore, the importance of identifying a live moving louse, nymph, or viable nit on the head for correct diagnosis cannot be stressed enough 15.

FIG. 2: HEAD LOUSE NIT

FIG. 3: HEAD LOUSE EMERGING FROM THE NIT
Life Cycle of Head Lice:
Nits/Eggs: Head lice begin their lives as eggs, or “nits.” The female adult head louse may lay an average of five eggs per day. 4 Eggs are attached singly to a hair shaft with a “glue” that is resistant to chemical and mechanical dislodgement Fig. 4. 16 Eggs are normally cemented to the shaft of the hair very close to the scalp. Nits are oval or teardrop-shaped and may range in color from white, yellow, or tan to gray, depending upon age and whether or not the egg has hatched or been killed by head lice treatments. It is thought that eggs attached to hairs greater than a one-quarter inch from the scalp have either already hatched, or will not hatch 17.
Nymphs: Eggs spend seven to ten days incubating close to the scalp before hatching to release the first nymphal stage Fig. 5. Nymphal stage head lice look very much like a miniature adult louse Fig. 6. The newly hatched nymph will crawl and seek a place to feed immediately. There are three nymphal stages punctuated by molting (the shedding of exoskeleton or “skin”). The three nymphal stages last about 8-12 days 18.
Adults: The final molt leads to an adult stage Fig. 6 where body growth stops, and sexual maturation occurs. Adult head lice continue to feed on blood every three to six hours. There are separate sexes in head lice, and females must mate and be fertilized to produce viable eggs. A mated female can continue to produce eggs for the duration of her life, which is about 30 days 19. She can lay an average of five eggs daily during this period. Until recently, the life cycle of the human head louse has been difficult to quantify because of environmental variance and the unavailability of in-vitro rearing systems. From a practical perspective, one can view the life cycle of Pediculus humanus var. capitis as follows: 20
- Egg without an eyespot (the eyespot indicating a developed nervous system)
- Egg from lay to hatch
- First nymphal (instar) stage to egg-laying adult.
In the context of a nonovicidal therapy, without considering pediculicide resistance, a “worst-case” scenario for therapy (or best case scenario for lice survival) is a life cycle with the longest time spent as an egg (12 days) and the shortest time spent as a non–egg-laying adult (8.5 days).
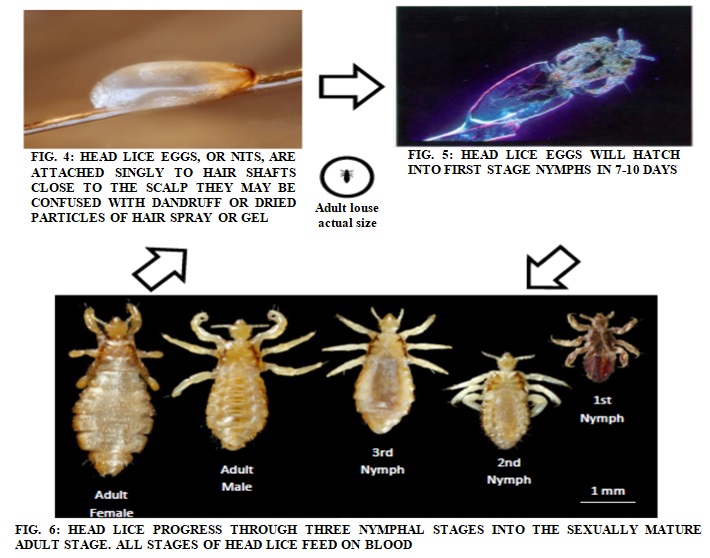

FIG. 7: LIFE CYCLE OF LICE
Until recently, the life cycle of the human head louse has been difficult to quantify because of environmental variance and the unavailability of in-vitro rearing systems. From a practical perspective, one can view the life cycle of Pediculus humanus var. capitis as follows: 21
- Egg without an eyespot (the eyespot indicating a developed nervous system).
- Egg from lay to hatch.
- Firstnymphal (instar) stage to egg-laying adult.
In the context of a nonovicidal therapy, without considering pediculicide resistance, a “worst-case” scenario for therapy (or best case scenario for lice survival) is a life cycle with the longest time spent as an egg (12 days) and the shortest time spent as an anon-egg-laying adult (8.5 days) 22.
Transmission of Head Lice:
Head Lice are Transmitted by:
Person-to-Person Transmission (Direct Contact): The majority of transmissions of head lice occur by direct head-to-head contact with an infested person. Most of the time, this is a close friend or relative 23.
Vector Transmission (Indirect Contact): This type of transmission may occur through the sharing of bedding, or by using personal items such as combs, brushes, scarves, hair ornaments, or hats of an infested person 24. Although transmission via indirect contact is possible, it is rare.
Common Ways of Transmission Through Head-to-Head Contact Include:
- Slumber parties
- Shared beds
- Sport activities
- Reading circles
Without Head-to-Head Contact, These Ways of Transmission are Highly Unlikely:
- School buses
- Hats, helmets, or headphones
- Gym mats
- Sitting at a desk
Anyone can get head lice, but some people are at greater risk than others. Those people include:
- Children between the ages of 3 and 11 years.
- Girls are more likely to get head lice than boys, possibly because of their play styles and sharing of personal items.
- People with long or short hair can contract head lice. Although all races can get head lice, studies show that children of African-American descent are less likely to become infested.
Symptoms of Head Lice: Parents, teachers, and other caregivers should be aware of the signs and symptoms of a head lice infestation because young children may not be able to express their discomfort directly. The following symptoms should raise the level of suspicion for a head lice infestation:
Itching (“pruritis”): Caused by an allergic reaction to lice bites. When lice feed, they inject a small amount of saliva into the skin. Over time, the host can develop an immune reaction to the saliva, which results in inflammation and itching. It may take four to six weeks for this reaction to occur in people infested for the first time. However, itching may not be present in all cases 25-26.
Sores on the Head: Rarely, scratching can lead to abrasions on the skin, allowing bacteria to enter and possibly lead to infection. In severe cases, lymph nodes around the head, neck, and underarms can become swollen.
Tickling Sensation: Lice movements in the hair may be felt by some infested individuals 27.
Sleeplessness and Irritability: Lice are more active at night, possibly disrupting sleep. Some people with head lice infestations have no symptoms. A lack of symptoms does not mean a lack of head lice 28.

FIG. 8: HEAD LICE INFESTATION MAY SOMETIMES BE CHARACTERIZED BY THE PRESENCE OF SCABS OR SCARS ON THE SCALP FROM ITCHING. IN THE ABOVE PHOTO, NITS ARE ALSO EVIDENT ON HAIR SHAFTS
General Therapeutic Considerations: Considerations in evaluating a lice therapy must include an understanding of a therapy’s mechanism of action and resistance, the prevalence of resistance, and safety. Application instructions also bear significance in light of the head lice life cycle. In the face of highly prevalent resistance to a particular molecule, therapy would likely be successful in only a small proportion of patients with lice infestations. Repeat treatments of resistant lice with preparations to which they are resistant will not kill the lice. In addition to wasting money, the patient is unnecessarily exposed to any associated toxicity of the therapy 29.
Putting aside the issue of resistance, a perfectly ovicidal and pediculicidal agent that acts on the louse nervous system requires 2 treatments separated at least 7 days apart. On day 0, all lice and eggs with eyespots would be killed. Those eggs without eyespots would develop eyespots by day 7 and thus be susceptible at that time. A solely pediculicidal agent would require 3 applications separated by 7 days Fig. 1. On day 0, all lice would be killed, leaving only newly laid eggs and eggs just about to hatch. Therapy on day 7 would kill those eggs that hatched. These nymphs would not have had time to mature to egg-laying adult.
What would remain are those eggs that are 7 days old but did not hatch. Therapy anytime between days 13 and 15 would kill the nymphs from those eggs, precluding development to egg-laying adult30.
Using average, rather than extreme, values for egg hatch (8.5 days10) and maturation time (9.7 days5, 10) lowers the demand for treatment by a solely pediculicidal agent to days 0 and 9 Fig. 2. Indeed, so long as the average time to hatch is less than the average time to mature to egg-laying adult, only 2 treatments are theoretically necessary. The challenge is to identify the time interval after which all eggs should be hatched, but before which new eggs are laid. The assurance of successful therapy is now at the mercy of favorable population statistics. Provided there is no resistance; enough lice may be killed to allow for stochastic extinction. These considerations become somewhat less relevant in the presence of resistant lice, which are not expected to respond regardless of treatment schedule 31-33.
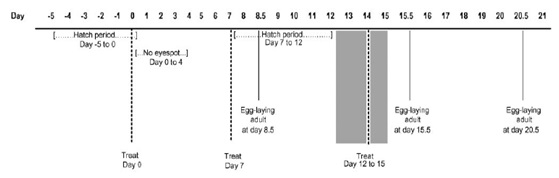
FIG. 9: GENERAL THERAPEUTIC CONSIDERATIONS
Worst-Case Scenario: Treatment at day 0 kills all lice, not in eggs. We are left with eggs laid just before therapy and eggs just hatched after therapy is washed away. For nonovicidal therapies, treatment must occur before each batch of hatched eggs matures to egg-laying adult. So, choosing day 7 gives a good buffer to the first deadline, which is day 8.5. We are left with eggs aged 7 and 12 days. We must treat before day 15.5 to kill day-7 hatchlings before they mature to egg-laying adult.
We must treat after day 12 to assure that all eggs have hatched before the last treatment. One could, theoretically, choose days 0 and 8 and then days 12 to 16.5, but treatment at day 0, week 1, and week 2 are easier to remember.
Average - Times Scenario: Treatment at day 0 kills all lice, not in eggs. We are left with eggs laid just before therapy and eggs just hatched after therapy is washed away. For nonovicidal therapies, treatment must occur before each batch of hatched eggs matures to egg-laying adult. In this case, all eggs will have hatched by day 8.5, but none will have matured to egg-laying adult until at least day 9.7. This leaves day 9 as the second and final therapy 34-35.
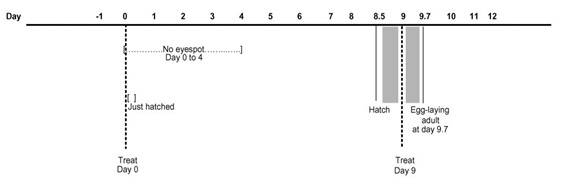
FIG. 10: WORST-CASE SCENARIO
Treatment of Head Lice: Every member of the household and all other close contacts should be examined. Treatment should be considered only if live lice or viable nits are observed. All clothing, towels, bed linens, stuffed animals, and cloth toys used by an infested child within 2 days before diagnosis should be washed in water hotter than 50 °C, or machine dried at the highest heat setting, for at least 30 minutes. Headgear, combs, headphones, and helmets should be cleaned and disinfected with a pediculicide or isopropyl alcohol. If none of those above modalities is plausible, sealing the objects in a plastic bag for 2 weeks is also an option to ensure decontamination. Floors, rugs, play areas, pillows, carpet squares, and upholstered furniture should be vacuumed to eliminate any shed hairs with viable eggs. The treatment should be directed at killing the lice and the ova. There are two effective basic treatment options for head lice:
Synthetic Drugs:
- Topical pediculicides
- Wet combing
- Oral therapy
Natural Drugs: Pediculicides are the most efficacious treatment for Pediculosis capitis. Agents with a long residual effect are more likely to be ovicidal. Treatment failures are often due to noncompliance, improper application of pediculicides, or reinfestation, and, rarely, resistance to pediculicides. Pediculicides are not recommended for children younger than 2 years.
Synthetic Drugs:
- Topical agents:
Pyrethrin: The treatment of choice for head lice infestation in the US is synthetic pyrethrin, 1% permethrin cream rinse. The hair is first shampooed with a non-conditioning shampoo and towel dried. After that, a 1% permethrin cream rinse is applied left on for 10 min and then rinsed off. Permethrin acts as a neurotoxin by disrupting the sodium channel current, causing delayed repolarization, and subsequent paralysis of the nerves in the exoskeletal muscle that allows the lice to breathe. Permethrin is the only pediculicide with a residual activity lasting for over 2 weeks. It is both pediculicidal and ovicidal. Therefore, one treatment is generally adequate. However, a second course, 7 to 10 days later, ensures a 95% cure rate. Resistance to 1% permethrin has been reported, but the prevalence of this resistance is unknown.
Pyrethrins Plus Piperonylbutoxide: These are manufactured from natural chrysanthemum extracts and are neurotoxic to lice. Natural pyrethrins have low mammalian toxicity but could cause a reaction in individuals that are allergic to chrysanthemums or ragweed. These over-the-counter products are mostly shampoos that are applied to dry hair and left on for 10minutes before rinsing out. None of the natural pyrethrins are completely ovicidal because newly laid ova lack a nervous system for the first 4 days. About 20% to 30% of the eggs remain viable after the first treatment. This requires reapplication 7 to 10 days later to kill newly emerged nymphs hatched from eggs that survived. The resistance of adult lice to these products has been reported.
Malathion (0.5%): This is an organophosphate (acetylcholinesterase inhibitor) that works by causing respiratory paralysis in the arthropod. This agent is a lotion that has to be applied to the hair, left to air dry, and washed off after 8 to 12 h. Malathion has high ovicidal activity, but the product should be reapplied if live lice are seen in 7 to 10 days. The major concerns are the high alcohol content of the product, making it highly flammable (hairdryers or curling irons should be avoided during treatment and the risk of severe respiratory depression in case of accidental ingestion. It should be used with extreme caution in cases in which resistance to other pediculicidal products is strongly suspected.
Permethrin (5%): This is a cream, available only by prescription in the US. This product is usually applied overnight for scabies. It is not currently approved by the Food and Drug Administration for use as a pediculicide. It has anecdotally been recommended for the treatment of head lice that appear to be refractory to other treatments. It is applied to the scalp and left on for several hours or overnight after which it should be rinsed off. No case-control studies have reported efficacy to date. One study suggested that lice resistant to 1% permethrin will not succumb to higher concentrations.
Crotamiton (10%): This is a lotion, available only by prescription in the US. It is not currently approved by the FDA and is used to treat scabies. A single study showed it to be effective against head lice when applied to the scalp and left on for 24 h before rinsing out. Safety and absorption in children, adults, and pregnant women were not evaluated.
Carbaryl (0.5%): This is a carbamate that binds to the same site on the acetylcholinesterase enzyme as organophosphates. In the UK in 1981, an open-label clinical study with 0.5% carbaryl lotion achieved a 100% cure rate in 81 participants. In 2000, an in-vitro survey showed prolonged survival of head lice with carbaryl exposure in one UK region. A follow-up, non-randomized, open-label clinical trial showed an 89% cure rate in this region compared with a 100% cure rate in another region. Carbaryl use is falling out of favor; based in part on evidence that it might be carcinogenic. The Department of Health in the UK acknowledges that carbaryl has mutagenic potential, and should continue to have restricted use only.
Lindane (1%): This is an organochloride that has central nervous system toxicity in humans. Several cases of severe seizures in children using lindane were reported. The use of lindane for treatment of lice or scabies was banned by California in 2002 due to concern over water supply contamination. It is available by prescription only, as a shampoo that should be left on for no more than 10 minutes, with repeated application in 7 to 10 days. It has low ovicidal activity, and resistance has been reported worldwide for many years. It should be used very cautiously. Lindane is contraindicated for pregnant or nursing women, in patients with seizure disorders, and patients with hypersensitivity to the product. The FDA has issued a public health advisory on the safety of lindane products. All topical pediculicides have to be rinsed from the hair over a sink, rather than in the shower or bath to limit exposure; and with cool water, to minimize absorption due to vasodilatation.
Pediculicide Resistance: None of the currently available topical pediculicides is 100% ovicidal, and resistance to all of them has been reported. A study conducted in the UK in 2000 concluded that there was high resistance to Permethrin, Phenothrin, and Malathion, with an 87% failure rate for Permethrin and a 64% failure rate for Malathion with the topical treatment. There are no reports of widespread Malathion resistance in the US. The prevalence of resistance is not known. When faced with a persistent case of head lice, several additional possible explanations must be considered, including misdiagnosis, noncomp-liance, re-infestation, lack of ovicidal or residual pediculicidal properties of the product, incorrect application, or resistance of lice to the agent.
Nit Removal after Treatment with a Pediculicide: Because none of the pediculicides are 100% ovicidal, manual removal of nits with a fine-toothed nit comb after treatment with any product is recommended. Nit removal can be difficult and time-consuming. Removal of nits with a louse comb is easier when the hair is wetted with water, or after shampooing or treatment with a conditioner. Some products are available that claim to loosen the “glue” that attaches nits to the hair shaft, making the process easier.
Vinegar or vinegar-based products (Clear Lice Egg Remover Gel) are intended to be applied to the hair for 3 minutes before coming out the nits. No clinical benefit has been demonstrated. 8% formic acid applied to wet hair for 10 min before coming out the nits has been shown to have some benefit in one study. Acidic solutions (pH 4.5–5.5) probably make the surface of the hair smoother, facilitating sliding the eggs off the hair. Neither of these products is recommended for use with permethrin because they may interfere with that product’s residual activity.
Wet Combing: Mechanical removal of lice with the use of wet combing is an alternative to insecticides. The rationale behind it is the fact that lice cannot move to another host within 7 days after hatching, and cannot reproduce within 10 days, and all eggs hatch within 7 to 10 days. The combing procedure is done on wet hair with added lubricant (hair conditioner or olive oil) and continued until no lice are found (15 to 30 minutes per session or longer for long, thick hair). Combing is repeated once every 2 to 3 days for several weeks and should continue for 2 weeks after any session in which an adult louse is found. This approach cured 38% of children in a trial conducted in 2000 in the UK, in which the treatment was carried out by parents, but it was only half as effective as Malathion treatment. However, in 2005, a new trial was conducted in the UK comparing the effectiveness of a current Bug Buster® kit with over-the-counter pediculicides containing Malathion or permethrin. The cure rate for wet combing with conditioner employing the Bug Buster® kit was found to be significantly greater than that for the over-the-counter pediculicides (57% v 13%).
Oral Agents:
Sulfamethoxazole/ Trimethoprim: These are used in otitis media doses was shown to be effective against head lice. This antibiotic is thought to kill the symbiotic bacteria in the gut flora of the louse; thereby interfering with its ability to synthesize Vitamin B. Death ensues from vitamin. In a recent study, this antibiotic demonstrated synergistic activity when used in combination with permethrin 1% when compared with permethrin 1% or sulfamethoxazole/ trimethoprim used alone. However, the treatment groups were small. Severe life-threatening allergic reactions, including Stevens-Johnson Syndrome and toxic epidermal necrolysis, despite being rare, making it an undesirable therapy if other alternatives exist. It is not currently approved by the FDA for use as a pediculicide. Several anti-helminthic agents, including ivermectin, levamisole, and albendazole, may be effective treatments for pediculosis capitis.
Ivermectin: This is an anti-helminthic agent structurally similar to the macrolide antibiotics, but without antibacterial activity. A single oral dose of 200 micrograms/kg, repeated in 10 days, was shown to be effective against head lice. This agent is also suggested as a good option for treatment of mass infestations. If ivermectin crosses the blood-brain barrier, it blocks essential neural transmission. Young children are at a higher risk for this adverse drug reaction. Therefore ivermectin should not be used for children that weigh less than 15 kg and in children younger than 5 years. This product is not currently approved by the FDA as a pediculicide.
Levamisole: A dose of 3.5 mg/kg once daily was suggested to be effective against pediculosis upon administration for 10 days.
Albendazole: A single dose of 400 mg, or a 3-day course of albendazole 400 mg, is effective against pediculosis capitis, with a repeated single dose of albendazole 400 mg after 7 days. No synergistic effect between albendazole and 1%permethrin was found. The use of these systemic treatments for head lice is only justified in severe infestation when topical treatments have failed or are ineffective.
Occlusive Agents: The use of a “petrolatum shampoo,” consisting of standard petroleum jelly massaged on the entire surface of the scalp and hair and left on overnight with a shower cap, was suggested to be effective. Thorough shampooing is required for the next 7 to 10 days to remove the entire residue. This thick substance obstructs the respiratory spiracles of the louse, preventing efficient air exchange, as well as the holes in the operculum of the eggs, resulting in death by suffocation. Another interpretation is that the intense attention to hair grooming results in removal of all the lice and nits. Hair pomades are easier to remove than petroleum jelly, but may not kill the eggs, and treatment should be repeated weekly for 4 weeks. Other occlusive substances have been suggested (mayonnaise, tub margarine, herbal oils, olive oil), but to date, only anecdotal information is available regarding their efficacy. During the past year, two new products for treating head lice were released in the UK: 4% dimethicone (Hedrin®) lotion and Full Marks® solution. These products act by coating the louse and disrupting its ability to manage water. Hedrin® was found to cure at least 70% of cases in two clinical trials. There is no clinical evidence to support Full Marks® product effectiveness yet.
A recent study suggests that Cetaphil® cleanser can be used as a dry-on, suffocation-based pediculicide lotion (NUVO® lotion), and is effective in the treatment of pediculosis capitis. However the study was anecdotal, not a well-designed randomized trial, and did not use a proper method to make the diagnosis of head lice infestation.
Head Lice Repellents: The insecticide residues left on hair shafts probably act as insect repellents even if the louse is resistant to the lethal effects of the insecticide. Piperonal is available as a head lice repellent spray. Lavender, citronella, and anise are also shown to be effective lice repellents in in-vitro studies. Citronella repellant formulation was found to be 3 to 4 times more effective than the placebo in protecting against head lice infestations.
Head lice infestation is associated with little morbidity but causes much anxiety, days lost from school and work, and millions of dollars spent on medications. Pediculosis capitis remains a prevalent disease that necessitates a multidisciplinary treatment approach. Adults should be aware of the signs and symptoms of head lice infestation; affected children should be treated promptly to minimize spread to others. The school or child care facility should be notified immediately so that additional cases can be detected and treated promptly. Chemical pediculicides should be used rationally and in conjunction with nonchemical treatment, modalities to prevent the emergence of resistance. Therapy rotation may also slow the appearance of resistant species. Healthy children should not be excluded from school due to head lice. The “no nit” policies for return to school needlessly keep many children out of school and create significant financial difficulties for their parents. These policies should be discouraged because they usually result in many children with non-viable it’s being kept out of school while asymptomatic children with active infestation remain in the classrooms. Because most children with nits alone will not become infested, excluding these children from school and requiring them to be treated with a pediculicide is unwarranted. Because most available pediculicides are incomplete ovicides, treating children with nits alone may not prevent subsequent infestation. Instead, children with nits alone should have regular follow-up examinations with lice comb during the following 14 days. Children with more than 5 nits within 0.7 cm of the scalp are at higher risk of becoming infested and may need more frequent follow- up examinations. Parental education programs help manage head lice. Only through improved understanding of the biology and physiology of the head louse can we effectively employ new and existing treatment modalities.
Natural Drugs:
Pongamia pinnata: arious extracts of Pongamia pinnata leaves were tested against the head louse Pediculus humanus capitis. Finding revealed that petroleum ether extracts possess excellent anti-lice activity with values ranging between 50.3% and 100% whereas chloroform and methanol extracts showed moderate pediculicidal effects. The chloroform and methanol extracts were also successful in inhibiting nymphs emergence, and the petroleum ether extract was the most effective with complete inhibition of emergence. Petroleum extract showed excellent activity due to the presence of triterpenoids.
Dichrostachys cinerea: Dichrostachys cinerea (Fam: Mimosaceae) known as Vurtuli in Hindi, Vidattalai in Tamil, Velantarah in Sanskrit and Sickle bush in English. The generic name ‘Dichrostachys’ means colored spikes. It is a much-branched thorny shrub, sometimes a small tree up to 2m in height. It is distributed throughout the dry and warm parts of India. Brushed young shoots used in the treatment of ophthalmia, astringent, rheumatism and urinary calculi, the leaves are used as fodder. The anti-lice activity of aqueous and ethanolic extract of Dichrostachys cinerea was studied. To provide a scientific basis for the traditional claim, it was compared with the marketed sample preparation. The ethanolic extract showed 98% mortality in 90 minutes. D. cinerea can be used in the herbal formulation as Pediculicidal agen.
Calpurnia aurea (Ait.): The genus Calpurnia (Leguminosae) comprises some seven species which are widely distributed in South Africa. Calpurnia aurea (Ait.) Benth is a yellow-flowered small tree or shrub (Natal Laburnum) widely distributed in Africa from Cape Province to Eritrea and which also occurs in Southern India.
Calpurnia aurea is used for the treatment of amoebic dysentery and diarrhea in animals, killing head lice in humans and ticks in animals, syphilis, diarrhea, leishmaniasis, tapeworm, trachoma, tinea capitis, wound, scabies, elephantiasis, and different swellings. In South Africa, Calpurnia leaves, and powdered roots are used to destroy lice and to relieve itches. Unspecified parts are used to destroy maggots, and the leaves are used to treat allergic rashes, particularly those caused by caterpillars. In East Africa, leaf sap is used to destroy maggots in wounds. In Nigeria, the seeds are used to treat abscesses. In Ethiopia, it is used to treat stomach complaints, headache, eye diseases, amoebic dysentery, scabies (skin infection caused by ticks) and as an insecticide.
Tagetes minuta: Tagetes minuta belongs to the family Asteraceae. T. minuta is rich in many secondary compounds including monoterpenes, sesquiterpenes, flavonoids, and Thiophenes. Because of the presence of these secondary compounds, T. minuta posses both insecticidal and anti-lice activity.
Azadirachta indica: Because topical compounds based on insecticidal chemicals are the mainstay of head lice treatment, but resistance is increasing, alternatives, such as herbs and oils are being sold to treat head lice. The seed extract of the neem tree was used and it was found to be the most effective than the other extracts of the neem tree.
Pyrethrin: The natural or synergized pyrethrins are a mixture of 6 active extracts from the flower heads of the ragweed relative Chrysanthemum zcineraria folium. Pyrethrins are usually available over the counter as a synergized formulation of 0.33% pyrethrin in 4% piperonyl butoxide. Pyrethrins blocks sodium channel re-polarization of the arthropod neuron, leading to paralysis and death. Pyrethrins are unstable in heat and light and have no residual activity after rinsing. Two applications of pyrethrins, separated by 1 week, are generally required because these agents are not ovicidal. Even with appropriate application, treatment failure has occurred.
CONCLUSION: In light of the review of therapeutic modes of action, resistance considerations, and head lice biology the number of new commercially available natural products for head lice has expanded over the last decade to a much greater extent than products containing defined chemical insecticides. However, the evidence on the efficacy of these new products based on published results of in vitro and clinical trials is markedly deficient. Evidence on safety is also deficient.
All over the counter, natural products should be supported by in-vitro data and well designed comparative therapeutic trials using head lice derived from the populations for whom the product is intended.
Since, the prevalence and degree of insecticide resistance of head lice to pyrethrin, permethrin and malathion are expected to increase, alternative topical therapies for pediculosis are needed. It is possible that, in the long run, plant extracts, or their constituent compounds, will replace chemical insecticides on the market.
ACKNOWLEDGEMENT: Nil
CONFLICT OF INTEREST: Nil
REFERENCES:
- Janniger CK and Kuflik AS: Pediculosis capitis. Cutis 1993; 51(6): 407-8.
- Frankowski BL and Weiner LB: American Academy of Pediatrics, Committee on School Health the Committee on Infections Diseases. Head lice Pediatrics 2002; 110: 638-43.
- Burkhart CN and Burkhart CG: Head lice: a scientific assessment of the nit sheath with clinical ramifications and therapeutic options. J Am Acad Dermatol 2005; 53(1): 129-33.
- Plastow L, Luthra M, Powell R, Wright J, Russell D and Marshall MN: Head lice infestation: bug busting vs. traditional treatment. J Clin Nurs 2001; 10(6): 775-83.
- Hansen RC and O’Haver J: Economic considerations associated with Pediculus humanus capitis Clin Pediatr (Phila) 2004; 43: 523-27.
- Maunder JW: Resistance to organochlorine insecticides in head lice, and trials using alternative compounds, Medical Officer 1971; 125: 27.
- Stichele RHV, Dezeure EM and Bogaert MG: Systematic review of clinical efficacy of topical treatments for head lice. BMJ 1995; 311: 604-08.
- Schachner LA: Treatment-resistant head lice: alternative therapeutic approaches. Pediatr Dermatol 1997; 14: 409-10.
- Burkhart CG, Burkhart CN and Burkhart KM: An assessment of topical and oral prescription and over-the-counter treatments for head lice. J Am Acad Dermatol 1998; 38: 979.
- Elston DM: Drug-resistant lice. Arch Dermatol 2003; 139: 1061.
- Picollo MI, Vassena CV, Cueto GAM, Vernetti M and Zerba EN: Resistance to insecticides and effect of synergists on permethrin toxicity in Pediculus capitis (Anoplura: Pediculidae) from Buenos Aires. J Med Entomol 2000; 37: 721.
- Hunter JA and Barker SC: Susceptibility of head lice (Pediculus humanus capitis) to pediculicides in Australia. Parasitol Res 2003; 90: 476.
- Mumcuoglu KY, Hemingway J and Miller J: Permethrin resistance in the head louse Pediculus capitis from Israel. Med Vet Entomol 1995; 9: 427-47.
- Burkhart CG and Burkhart CN: Safety and efficacy of pediculicides for head lice. Expert Opin Drug Saf 2006; 5: 169.
- Canyon D and Speare R: A comparison of botanical and synthetic substances used to prevent head lice. Int J Dermatol 2006.
- Mumcuoglu KY, Friger M, Ioffe-Uspensky I, Ben-Ishai F and Miller J: Louse comb versus direct visual examination for the diagnosis of head louse infestations. Pediatr Dermatol 2001; 18(1): 9-12.
- Di Stefani A, Hofmann-Wellenhof R and Zalaudek I: Dermoscopy for diagnosis and treatment monitoring of capitis. J Am Acad Dermatol 2006; 54(5): 909-11.
- Burgess IF: New developments in the treatment of head lice. Nurs Times 2006; 102(26): 45-6.
- Meinking TL, Taplin D, Kalter DC and Eberle MW: Comparative efficacy of treatments for Pediculosis capitis Arch Dermatol 1986; 122(3): 267-71.
- Elston DM: Drugs used in the treatment of pediculosis. J Drugs Dermatol. 2005; 4(2): 207-11.
- Yang YC, Lee SG, Lee HK, Kim MK, Lee SH, and Lee HS: A piperidine amide extracted from Piper longum fruit shows activity against Aedes aegypti mosquito larvae, J Agric Food Chem 2002; 50: 3765.
- Perrucci S, Cioni PL, Cascella, A and Macchioni F: Therapeutic efficacy of linalool for the topical treatment of parasitic otitis caused by Psoroptes cuniculi in the rabbit and in the goat. Med Vet Entomol 1997; 1111: 300.
- Roth GN, Chandra A and Nair MG: Novel bioactivities of Curcuma longa J Nat Prod 1998; 61: 542.
- Heukelbach J, Oliveira FA and Speare R: A new shampoo based on neem (Azadirachta indica) is highly effective against head lice in-vitro. Parasitol. Res 2006.
- Yang YC, Lee HS, Clark JM and Ahn YJ: Insecticidal activity of plant essential oils against Pediculus humanus capitis (Anoplura: Pediculidae). J Med Entomol 2004; 41: 699.
- Yang YC, Choi HY, Choi WS, Clark JM and Ahn YJ: Ovicidal and adulticidal activity of Eucalyptus globulus leaf oil terpenoids against Pediculus humanus capitis (Anoplura: Pediculidae). J Agric Food Chem 2004; 52: 2507.
- Yang YC, Lee SH, Lee WJ, Choi DH and Ahn YJ: Ovicidal and adulticidal effects of Eugenia caryophyllata bud and leaf oil compounds on Pediculus capitis. J Agric Food Chem 2003; 51: 4884.
- Morsy TA, Ela RG, Nasser MM, Khalaf SA and Mazyad SA: Evaluation of the in-vitro pediculicidal action of four known insecticides and three medicinal plants extracts. J Egypt Soc Parasitol 2000; 30: 699.
- Tiangda CH, Gritsanapan W, Sookvanichsilp N and Limchalearn A: Anti-headlice activity of a preparation of Annona squamosa seed extract. Southeast Asian J Trop Med Public Health 2000; 31(1): 174.
- Sparks TC, Crouse GD and Durst G: Natural products as insecticides: the biology, biochemistry and quantitative structure-activity relationships of spinosyns and spinosoids. Pest Manag Sci 2001; 57: 896.
- Van der Stichele RH, Dezeure EM, and Bogaert M.G: Systematic review of clinical efficacy of topical treatments for head lice. Br Med J 1995; 311: 604.
- Chopade VV, Tankar AN, Pande VV, Tekade AR, Gowekar NM, Bhandari SR and Khandake SN: Pongamia pinnata: Phytochemical constituents, traditional uses and pharmacological properties: A review. Int J Green Pharm 2008; 2: 72-75.
- Jeba A, Samuel J and Radhamani S: In-vitro screening of anti-lice activity of Pongamia pinnata leaves, Korean Journal of Parasitology 2009; 47(4): 377-80.
- Breuer M, Hoste B, De Loof A and Naqvi SNH: Effect of Melia azedarach extract on the activity of NADPH-cytochrome c reductase and cholinesterase in insects. Pestic Biochem Physiol 2003; 76: 99-03.
- Singh D, Garg G and Gupta V: In-vitro screening of Mucuna pruriens seeds extract for anti-lice activity. Pharma and Bio Sciences 2011; 2(3): 107-10.
How to cite this article:
Bharti SN, Umekar MJ and Duragkar NJ: A review on Pediculus humanus capitis based on life cycle, resistance, safety considerations and treatment. Int J Life Sci & Rev 2017; 3(2): 13-24. doi: 10.13040/IJPSR.0975-8232.IJLSR.3(2).13-24.
All © 2015 are reserved by International Journal of Life Sciences and Review. This Journal licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 3.0 Unported License.
Article Information
1
13-24
897
1624
English
IJLSR
S. N. Bharti *, M. J. Umekar and N. J. Duragkar
Smt. Kishoritai Bhoyar College of Pharmacy, New Kamptee, Nagpur, Maharashtra, India.
shankarbharti10@gmail.com
21 January 2017
18 February 2017
21 February 2017
10.13040/IJPSR.0975-8232.IJLSR.3(2).13-24
28 February 2017