


ASSESSMENT OF FUNCTIONAL ABILITY AND MOBILITY AMONG SENIOR CITIZENS
HTML Full TextASSESSMENT OF FUNCTIONAL ABILITY AND MOBILITY AMONG SENIOR CITIZENS
T. Vidhya * 1 and S. Punitha Josephine 2
Meenakshi College of Nursing 1, Mangadu, Chennai - 600069, Tamil Nadu, India.
Karpagavinayaga College of Nursing 2, Kanchipuram - 603308, Tamil Nadu, India.
ABSTRACT: Background: The population of senior citizens is progressively increasing worldwide due to various factors. As age increases, it causes numerous changes in the functional ability and mobility among senior citizens. Objectives: Assess the level of functional ability and mobility among the senior citizens, correlate the functional ability and mobility among the senior citizens, associate demographic variables with functional ability and mobility. Materials and Methods: The non-experimental research approach of the descriptive design was adopted. The study was conducted at a selected rural community in Bangalore with a sample size of 100. The study participants were selected using a purposive sampling technique of those who fulfill the inclusion criteria. Katz Index of Independence in Activities of Daily Living (ADL), Lawton’s Instrumental Activities of Daily Living (IADL) and TINETTI Performance Oriented Mobility Assessment tool (POMA) (balance and gait) scales were used to collect the data. The collected data were analyzed using descriptive and inferential statistics. Results: Most of the samples (95%) were independent to perform their ADL. 91.3% of females and 86.5% of males were dependent in terms of instrumental activities of daily living. Distribution of mobility revealed that 81% of samples were in less chance of fall, and only 6% of samples were at high risk of fall. There was a positive correlation between functional ability and mobility. This implied that as ADL and IADL increase mobility also increases among senior citizens. This correlation was statistically significant at level p<.001 and <.01, respectively. There was a significant association of IADL with demographic variables such as the history of illness, vision, hearing acuity at p< .05 and that of age at p<.01 respectively. Conclusion: Nurses are playing a greater role to assess the needs of the senior citizens and provide the prioritized care for a harmonious life.
Keywords: Senior citizens, Activities of daily living (ADL), Instrumental activities of daily living (IADL), Mobility, Elderly
INTRODUCTION: In every country, the proportion of people aged over 60 years is growing faster than any other age group as a result of both longer life expectancy and declining fertility rates due to the advancement in the health care industry.
Normal aging changes reduces the functional ability and mobility of senior citizens. Functional mobility includes activities of daily living (ADL) and instrumental activities of daily living. ADL refers to daily self-care activities within an individual’s place of residence, in outdoor environments or both.
IADL are not necessary for fundamental functioning, but they let an individual live independently in the community. ADL include bathing, dressing, toileting, transferring, eating, and controlling bladder and bowel.
IADL enables the people to experience a good quality of life and encompasses (activities like) using a telephone, shopping, preparing meals, doing housework (chores), washing clothes, travelling on own, taking drugs, and managing finances. The basic activities, such as rising from a chair, performing the task that involves unsupported standing, etc., are required for better to maintain their functional ability. The prevalence rate of inability to perform ADL, IADL, and impairment of mobility is high among senior citizens, and it rises steeply with advancing age and is especially high for persons aged 85 and over 1.
Aging, which is an inescapable reality of human existence on the planet earth plays a crucial role in the global demographic transition. According to the US Census Bureau report (2015), there are great variations in the older population within the less developed world as well. Asia stands out as the population giant, given both the size of its older population (617.1 million in 2015) and its current share of the world older population (more than half). By 2050, almost two-thirds of the world’s older people will live in Asia 2.
The population of aging had been increased in India since 1961 due to a sharp decline in death rates accompanied by an increasing expectation of life at age 60. The 2001 census had shown that the senior citizen population of India accounted for 77 million. It is projected to become 2 billion by 2050 3.
China and India are currently having the largest number of older people, about 109 million and 62 million respectively. By 2050 both countries are projected to have the 65-year-old and older population of about 350 and 240 million respectively 4.
Aging causes numerous changes in the physiology of human being, which decreases the functional ability and mobility. Major changes include sensory perceptual alteration and impairment of balance and gait. Most of the senior citizens suffer from chronic illness, degenerative diseases, which ultimately decrease the functional capacity and mobility. This, in turn, makes them dependent on caregivers. Inadequate care results in falls and depression among senior citizens. A national long term survey conducted by Kasper et al., (2000) regarding ADL among elderly reported that 3 million were with impairments in one or more ADL 5. Thus, it is the prime responsibility of the nurses to assess the functional ability and mobility, thereby to develop insight on the needs of the senior citizens.
Statement of the Problem: A study to assess the functional ability and mobility among senior citizens at selected rural area in Bangalore.
Objectives:
- Assess the level of functional ability and mobility among the senior citizens.
- Correlate the functional ability and mobility among the senior citizens.
- Associate demographic variables with functional ability and mobility.
MATERIALS AND METHODS: The non-experimental research approach of descriptive design was adopted. The study was conducted at a selected rural community in Bangalore. By using purposive sampling technique, a total of 100 senior citizens, both male, and female of age 60 and above, those who can understand Kannada were included for the study.
Similarly, senior citizens, those were physically, mentally challenged, and fracture limbs during the study period were not included for this study. The interview method was adopted for part I, II, and III. The investigator instructed the subjects to perform Part IV - Balance and Gait test and scored accordingly.
Description of the Tool and Scoring: The structured tool comprised of four parts
Part I: Demographic Variables: This included 14 items such as Age, Gender, Marital status Religion, Educational qualification, Type of house, Type of family, Size of family, Income History of fall, History of illness, Visual acuity, and Hearing acuity.
Part II: Katz Index of Independence in Activities of Daily Living (ADL): 6, 7 This was used to assess the performance of daily living which encompassed six functions namely Bathing, Dressing, Toileting, Transferring, controlling bladder and bowel and feeding. Each item was scored Yes/No for independent performance. The maximum and minimum score of the tool were 6 and 0, respectively.
Part III: Lawton’s Instrumental Activities of Daily Living (IADL): 8, 6, 9, 10 This is a reliable and valid tool (r = 0.85) to assess the independent living skills of senior citizens. The eight domains of the tool were namely Using the telephone, Getting to places beyond walking distance, Grocery shopping, Preparing meals, Doing house chores, Doing laundry, Taking medications, and Managing money. Each item was scored ranging from 0 - 2 with the overall score of maximum 16 for women and 10 for men. The areas of food preparation, housekeeping, and laundry were excluded for men. The senior citizens independent living skills were scored according to their highest level of functioning in that category based on self-reported information.
A summary score ranged from “0” low function, dependent, 1 to 16 high function, independent for women and “0” through 10 for men. The total scores categorized as for Women: 0 low function and dependent, 1-07 moderate function and dependent, 8 - 16 - high function and independent. For Men: 0 low function and dependent, 1-5 moderate function and dependent, 6-10 high function and independent.
Part IV: Assessment of Mobility was done by TINETTI Performance Oriented Mobility Assessment tool (POMA). It consisted of balance and gait tests
Part-A: Balance Test: This included 9 items; each item was scored according to the senior citizen’s maximum ability to balance. The maximum score of each item was 2, and the minimum was 0 except item 1, 7 which had a maximum score of 1.
Part-B: Gait Test: This included 7 items. The senior citizen’s maximum ability to walk at “Usual Pace,” “Rapid but Safe” pace using usual walking aids were scored. The maximum score of each item was 2, and the minimum was 0 except the item numbers 10, 11, 12, 13, 16 which were scored a maximum of 1. A total score of both balance and gait test were computed for mobility with a maximum of 28. It was categorized as< 12 high risks for fall, 12-19 greater chance of fall, >20 less chance of fall.
Findings:
TABLE 1: DISTRIBUTION OF DEMOGRAPHIC VARIABLES AMONG SENIOR CITIZENS; N=100
| S. no. | Demographic Variables | No | % |
| 1 | Age in Years | ||
| 60-65 yrs | 53 | 53 | |
| 66-70 yrs | 25 | 25 | |
| 71-75 yrs | 6 | 6 | |
| 76-80 yrs | 10 | 10 | |
| 81 and above | 6 | 6 | |
| 2 | Sex | ||
| Male | 46 | 46 | |
| Female | 54 | 54 | |
| 3 | Religion | ||
| Hindu | 47 | 47 | |
| Christian | 2 | 2 | |
| Muslim | 51 | 51 | |
| 4 | Educational qualification | ||
| Illiterate | 72 | 72 | |
| Primary | 19 | 19 | |
| Middle | 9 | 9 | |
| 5 | Type of House | ||
| Pucca | 56 | 56 | |
| Kachcha | 39 | 39 | |
| Thatched | 5 | 5 | |
| 6 | Type of Family | ||
| Joint | 64 | 64 | |
| Nuclear | 36 | 36 | |
| 7 | No. of Family members | ||
| 2--4 | 40 | 40 | |
| 5--7 | 20 | 20 | |
| 8--10 | 29 | 29 | |
| > 10 | 11 | 11 | |
| 8 | Marital status | ||
| Married | 1 | 1 | |
| Single | 68 | 68 | |
| Divorcee | 29 | 29 | |
| Widower | 2 | 2 | |
| 9 | Vision | ||
| Normal | 25 | 25 | |
| Impaired | 75 | 75 | |
| 10 | Hearing Acuity | ||
| Normal | 11 | 11 | |
| Impaired | 89 | 89 |
TABLE 2: LEVEL OF ACTIVITIES OF DAILY LIVING AMONG SENIOR CITIZENS; N=100
| Level of activities of daily living | Frequency | % |
| Severe functional impairment | 1 | 1.0 |
| Moderate
impairment |
4 | 4.0 |
| Full
function |
95 | 95.0 |
TABLE 3: LEVEL OF INSTRUMENTAL ACTIVITIES OF DAILY LIVING AMONG SENIOR CITIZENS; N=100
| Level of instrumental activities of daily living | Male n=46
|
Female n=54 | ||
| Frequency | % | Frequency | % | |
| Low function and dependent | 1 | 2.17 | 0 | 0 |
| Moderate function and dependent | 5 | 10.86 | 12 | 28.57 |
| High function and dependent | 40 | 86.5 | 42 | 91.30 |
Majority of the samples (95%) were independent to perform their ADL. 91.3% of females and 86.5% of males were dependent in terms of instrumental activities of daily living.
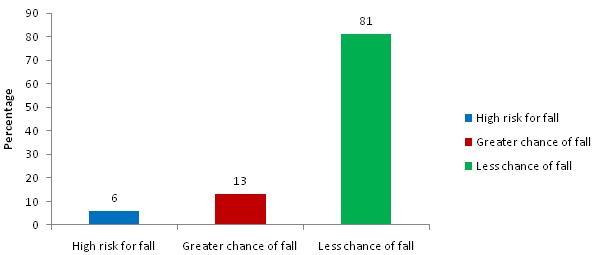
FIG. 1: LEVEL ON MOBILITY AMONG SENIOR CITIZEN
TABLE 5: CORRELATION OF ACTIVITIES OF DAILY LIVING WITH MOBILITY AMONG SENIOR CITIZENS
| Variables | Mean | Std.
Deviation |
r - value | P
value |
| Activities of daily living | 5.7000 | .70353 | .426*** |
.000 |
| Mobility | 22.4200 | 5.31470 |
***significant at level p< .001
There was a positive correlation between functional ability and mobility. This implied that as ADL and IADL increase mobility also increases among senior citizens. This correlation was statistically significant at level p<.001 and <.01, respectively.
TABLE 6: CORRELATION OF INSTRUMENTAL ACTIVITIES OF DAILY LIVING WITH MOBILITY AMONG SENIOR CITIZENS
| Variables | Mean | Std. Deviation | r - value | P
value |
| .308** | .002 | |||
| Instrumental activities of daily living
Mobility |
0.71
22.4200 |
3.26
5.31 |
** Significant at level p<.01
There was a positive correlation between functional ability and mobility. This implied that as ADL and IADL increase mobility also increases among senior citizens. This correlation was statistically significant at level p<.001 and <.01, respectively. There was a significant association of IADL with demographic variables such as the history of illness, vision, hearing acuity at p<.05 and that of age at p<.01 respectively. There was a significant association of mobility with demographic variables such as age, history of fall, diseases, vision and marital status at p<.05 respectively and the type of family at p<.01.
DISCUSSION: Most of the senior citizens (95%) were independent to perform their ADL. This finding is consistent with the study conducted by Dewen Wang et al., (2009), which disclosed that the elderly persons were dependent on others as their ADL scores were declined 11. Lariane Mortean Ono et al., (2015) stated that when the senior citizens are physically active, there is less chance for functional disability 12.
The majority (82%) of the senior citizens functions the IADL independently, and distribution of mobility showed, 81% of samples were in less chance of fall and only 6% samples were in high risk of fall. Similarly, Suzuki N et al., (2009) examined the changes in instrumental activities of daily living among community-dwelling elderly. It depicted that 75.6% of the elderly were good at performing IADL. Within a year, 21.1% and 3% of the elderly shifted to borderline and low performance of IADL respectively.
They also found that the borderline performance elderly had significantly lower mobility and IADL 13. As age-related changes are progressive the functional ability and mobility of the senior citizens may decline in the future course of time, which increases the risk of fall, and they may become dependent. Consequently, this increases the burden to the caregiver, in turn, this may increase the population of institutionalized senior citizens. There was a positive correlation between functional ability and mobility. This implied that as the senior citizens were in less chance for fall, they were more independent to carry out their ADL and IADL. This correlation was statistically significant at p<.01 Level respectively. This finding enhances the knowledge of the nurses to develop the strategies to promote mobility and thereby to perform ADL, IADL independently.
Implications: The findings of the study imply that the nursing curriculum should be re-framed adequately to meet the demands of the ever-growing population of a senior citizen. The clinical practice for the students in gerontological nursing should enrich their skill in rendering quality nursing care to the geriatric population. Nursing research should be conducted to bring innovative nursing practice.
CONCLUSION: In almost every country, the proportion of people aged over 60 years is growing faster than any age group, as a result of both longer life expectancy and declining fertility rates. As the aging population increases, it exerts greater demand on nurses to develop insight on gerontological nursing, thereby to meet the needs of the society. It also challenges society to adapt, to maximize the health and functional capacity of older people as well as their social participation and security.
ACKNOWLEDGEMENT: Nil.
CONFLICT OF INTEREST: Nil.
REFERENCES:
- S. Bureau of the Census. Current Population Reports.1022. Washington: U.S. Government Printing Office; Mar. 1988. United States population estimates by age, sex, and race 1980-1987; 25.
- US Census Bureau: An Aging world 2015, International population reports 2016; 5/16-1.
- Census of India 1961-2001.
- US Census Bureau: An aging world 2008, International population reports 2009; 5/16.
- Kasper JD, Shore A and Penninx BWJH: Care giving arrangements of older disabled women, care giving preferences, and views on the adequacy of care. Aging (Milano) 2000; 12(2): 141-53.
- Lawton MP and Brody EM: Assessment of older people: Self-maintaining and instrumental activities of daily living. Gerontologist 1969; 9: 179-86.
- Gallo JJ and Paveza GJ: Activities of daily living and instrumental activities of daily living assessment. In Gallo JJ, Bogner HR, Fulmer T and Paveza GJ: Handbook of Geriatric Assessment, MA: Jones and Bartlett Publishers. 4th ed., 2006: 193-40.
- Graf C: The Lawton Instrumental Activities of Daily Living Scale. AJN 2008; 108(4): 52-62.
- Lawton MP, Moss M, Fulcomer M and Kleban MH: Multi-level assessment instrument manual for full-length MAI. North Wales PA: Polisher Research Institute, Madlyn and Leonard Abramson Center for Jewish Life 2003.
- Pearson V: Assessment of function. In Kane R and Kane R (Eds.): Assessing Older Persons. Measures, Meaning and Practical Applications. New York: Oxford University Press 2000: 17-48
- Wang D, Zheng J, Kurosawa M, Inaba Y and Kato N: Changes in activities of daily living (ADL) among elderly Chinese by marital status, living arrangement, and availability of healthcare over 3 years. Environ Health Prev Med 2009; 14(2): 128-41.
- Ono LM, Schneider IJC, Confortin SC and D’ Orsi E: Paid work and physical activity preserve functional capacity in elderly people. Gerontol Geriatr Med 2015; 1.
- Suzuki N, Goto A, Yokokawa H and Yasumura S: Changes in ability and performance-based IADL among community-dwelling elderly, Nihon Ronen Igakkai Zasshi. Japanese Journal of Geriatrics 2009; 46(1): 47-54.
How to cite this article:
Vidhya T and Josephine SP: Assessment of functional ability and mobility among senior citizens. Int J Life Sci & Rev 2017; 3(8): 87-91. doi: 10.13040/IJPSR.0975-8232.IJLSR.3(8).87-91.
All © 2015 are reserved by International Journal of Life Sciences and Review. This Journal licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 3.0 Unported License.