


LEVEL OF SIALIC ACID IN ORAL CANCER PATIENTS
HTML Full TextLEVEL OF SIALIC ACID IN ORAL CANCER PATIENTS
D. Madhumathi
Saveetha Dental College and Hospitals, 162, Poonamalle High Road, Velappanchavadi, Chennai - 600077, Tamil Nadu, India.
ABSTRACT: Aim And Objective: This review aims to find the sialic acid level in oral cancer patients. Background: Oral cavity cancer is currently the most frequent cause of cancer-related death among Indian men. It is preceded by oral precancerous conditions like leukoplakia or oral sub mucous fibrosis. Altered cell surface topography is the soul of the malignant cell. Early detection is the key to treat oral cancer. Attempts are on to develop sensitive, specific, and reliable biochemical tests for early detection and diagnosis. Glycoproteins and Glycolipids are important constituents of the cell membrane; hence, they play an important role in malignancy. Glycoconjugates are released into the circulation in increased level from malignant cells due to increased turnover, secretion, or shedding of malignant cells. So the measurement of and salivary glycoprotein and glycolipids has received a wide range of acceptance in the screening of oral cancer. Sialic acid is N-acetyl neuraminic acid. It is a negatively charged nine-carbon monosaccharide commonly attached to carbohydrate chains of glycoproteins and glycolipids. Salivary glycoproteins play an important role in the properties and functions of saliva. So estimate the amount of sialic acid in saliva provide food for the biochemical marker to diagnose oral cancer.
Keywords: Sialic acid, Tumour marker, Oral cancer, Tobacco, Glycoconjugates
INTRODUCTION: Saliva is a complex fluid which is a secretion from the oral cavity. It composed of a wide variety of organic and inorganic constituents, which helps to maintain the oral environment. The role of sialic acid in aberrant glycosylation, including sialylation in the cell membrane are the major events in malignant transformations 1. Recent studies have reported that the maximum levels of total sialic acid in various malignancies.
A higher concentration of sialic acids is present as a component of glycolipids and glycoproteins2. These glycoproteins and glycolipids are collectively called as Glycoconjugates, which plays an important role in malignant transformations 3, 4.
Oral cancer is the most common cancer-related deaths in all countries. Oral cancer is caused by oral pre-cancerous conditions like sub-mucous fibrosis or leukoplakia 5. Most commonly, oral cancer is caused by tobacco chewing, smoking, etc. 5 Sialic acid is an N-acetyl neuraminic acid which is a negatively charged nine-carbon monosaccharide, and it is attached by an alpha glycosidic linkage to the residues of glycoproteins and glycolipids sialic acids are the components of glycoprotein and glycolipids which are called as a Glycoconjugates 6. Glycoconjugates plays a major role in malignant transformations. The incorporation of sialic acid into Glycoconjugates by using cytidine monophosphate (CMP) takes place in the golgi apparatus7. Sialic acid is a moiety of a carbohydrate epitope which is important for biological interaction including cell adhesion. So, the sialic acid is an important constituent in changing the characters of transformed cells. This will initiate the changes in glycoproteins at an early stage of tumourigenesis 8.
Structure of Sialic Acid: The sialic acid family includes 43 derivatives of the nine-carbon sugar neuraminic acid, but these acids unusually appear free. Normally they can be found as components of oligosaccharide chains of mucins, glycoproteins and glycolipids occupying terminal, non reducing positions of complex carbohydrates on both external and internal membrane areas where they are very exposed and develop important functions9.
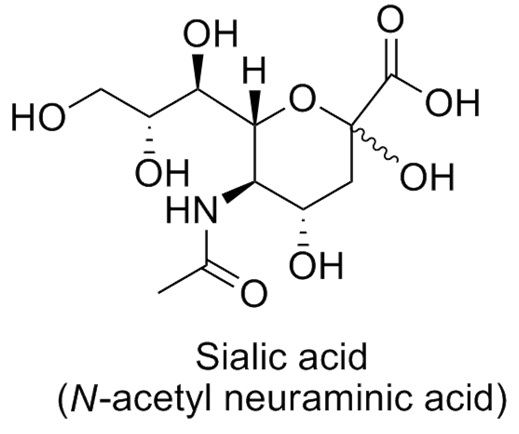
FIG. 1: STRUCTURE OF SIALIC ACID
Sialic acid is a terminal sugar unit of oligosaccharides of glycoproteins and glycolipids which are the constituents of cell surface 10. They enter the circulation by shadding the cell surface. Terminal sugars of glycoproteins and Glycolipids plays an important role in the development of cell adhesion and also in the cell to cell interaction, which is significant in the malignant transformations 10. The precursor for the synthesis of sialic acid is glucose 7. Uridine -diphosphate-N-acetyl-D-glucosamine is formed as an intermediate in the reaction. And this above step was inhibited by the feedback inhibition 7. Finally, the sialic acid is produced from N-acetylmannosamine (ManNAc) through the intermediate compounds such as N-acetylmannosamine-6-phosphate and N-acetyl neuraminic acid-9-phosphate 7. The numbering of the sialic acid structure initiates at the carboxylate carbon and continues around the chain. The configuration which places the carboxylate in the axial position is the alpha-anomer 7.
Bio-Synthesis of Sialic Acid: The term sialic acid is a derivative of neuraminic acid. There is more than 20 natural neuraminic acid are present. Sialic acid belongs to the family of nine carbon alpha-keto acids. The two main enzymes which are responsible for the biosynthesis of the sialic acid are UDP-N-acetylglucosamine 2-epimerase and Sialic acid synthase 10. Sialic acid is synthesized by glucosamine -6-phosphate and acetyl CoA through transferase, resulting in the production of N-acetyl glucosamine-6-phosphate 11, 12.
Through epimerization, it reacts with phosphoenolpyruvate to become N-acetyl neuraminic acid-9-phosphate 11, 12. Sialic acids are the most important molecules of life because they occupy the terminal position on macromolecules and cell membranes, and they involved in many biological and pathological phenomena. The structures of sialic acids, composed of over 40 neuraminic acid derivatives 13.
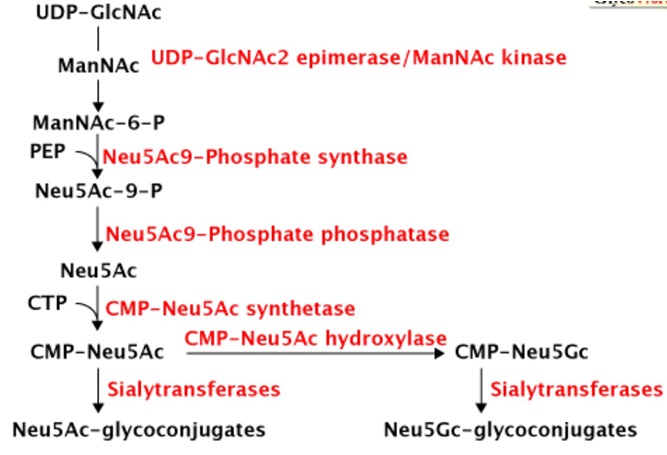
FIG. 2: BIO-SYNTHESIS OF SIALIC ACID
Sialic Acid as a Tumour Marker: Sialic acid is related to tumor cells due to increased sialylation and sialyltransferase activity 14. Focusing on sialic acid as a tumor marker is examined from the perspective aberrant glycosylation in cancer cell membranes, which results in the activation of a new glycosyltransferase, which are the characteristics of tumor cells. The increased amount of sialic acid on the surface of tumor cells is due to an increase in the adhesion contributed to the organization of larger tumor cells 14. Sialic acid is a terminal sugar unit of Glycoproteins and glycolipids which are called as Glycoconjugates. That Glycoconjugates plays an important role in malignant transformations in humans 10. During malignant transformation, the main change occurs in the Glycoconjugates, which increases the size of oligosaccharides and the sialic acid enters the terminal portion10. The incorporation of sialic acid at a terminal position of sugar units will determine the surface characteristics of the cell and secreted glycoproteins 10. The entry of sialic acid at the terminal portion suggests that sialylation is dominant in tumor cells. Sialyltransferase activities will determine the extent of sialylation of Glycoconjugates. Any elevations in the sialyltransferase activity can be seen in the cancer patients 10, 11.
Sialic acid also acts as a tumor cell metastasis, which is a development of secondary malignant growth at a distance from a primary site of cancer and this ability is related to total sialic acid in culture 15. When sialic acid molecules are exposed on the tumor cell surface, the extend to the sialylation of galactosyl and N-acetyl galactosaminyl residues present on the cell surface of oligosaccharide chains. The tumor cells which has a heavily sialylated surface to evade recognition by immune surveillance, which facilitates the metastatic spread. The increased amount of sialic acid on the tumor cell surface is due to the increase in the adhesiveness which contributes to the formation of larger tumor emboli16.
Sialic Acid in Oral Tumour: Oral cell cancer is the common form of oral cancer, and it has high mortality rates 16. The most important diagnostic challenge to detect cancer is the changes in the mucosa. This could be done by detecting the damage to DNA at a very early stage. The carcinogenic effects on cellular material are measured as genotoxicity, which quantitates the potential of a particular environment (chemical/ electromagnetic) to cause damage to the DNA of a cell 16. And also the advanced method for detecting DNA damage includes the measurement of genotoxic chemical levels, their derivatives, and metabolites in body fluids. The biochemical tests for oral cancer include the detection of all carcinogenic agents present in the tobacco like Benzo[a]pyrene, ethyl carbamate, volatile aldehydes, nitrosamines, and nitrosamine acids 16.
A micronuclei assessment is a marker for genotoxic damage in the assessment of nuclear changes in tobacco users as well as in the development of pre-malignancies. In premalignancy conditions, there was an increase in salivary free and protein-bound sialic acid levels, but once the malignancy developed the serum-free sialic acid was increased first which is followed by increased levels of serum protein-bound sialic acid117.
This is explained by the carcinogenic action of tobacco on oral epithelium16. Epithelial exposure to tobacco leads to genotoxic damage in premalignant lesions where the alterations to glycoconjugates are less severe, resulting in the detection of sialic acid only in saliva. Carcinogens alter the other structures of the cell such as cytoplasmic cell membrane molecules 16. Assessment of total serum/ salivary sialic acid is a successful tool to predict the development of precancer and cancer as the sialic acid spills into circulation/ saliva 17.
CONCLUSION: Sialic acid is the most sensitive marker of tumor marker. Levels of free and protein-bound salivary sialic acid in leukoplakia and oral cancer patients indicate the importance of tumor marker. Saliva and sialic acid both are responsible for the development of oral cancer. This review reveals that the elevations in the sialyltransferase activities can be seen in the cancer patients. More understandings of the role in glycosylation, especially sialylation, for cancers will offer a different idea in managing the cancers in the future.
ACKNOWLEDGEMENT: Nil
CONFLICT OF INTEREST: Nil
REFERENCES:
- Wang PH: Altered glycosylation in cancer-Sialylation and sialyltransferases. Journal of Cancer Molecules 2005; 1(2): 73-81.
- Mizanur RM and Pohl: Sialic acid synthesis and signaling. Biofiles Glycobiology 5(1): 13.
- Kanduma EG, Mukuria JC and Mwanda OW: Serum total sialic acid and Hanganutziu-Diecher antibody in normals and in cancer patients. 2007; 84(5): 21.
- Romppanen J: Serum sialic acid as a marker of alcohol consumption: effect of liver disease and heavy drinking. Alcohol Clin Exp Res 2002; 26(8): 1234-8.
- Dhiraj JT, Chhaya D, Kaveri T, Hallikeri and Udupa R: Salivary sialic acid as a marker of oral cancer. 2014; 1(1): 11-16.
- Tanner ME: An enzymes of biosynthesis of sialic acids. Bioorganic Chemistry 2005, 33(3): 216-228, doi:10.1016/ j.bioorg.2005.01.005
- Alhadeff, Domino, Hiraiwa, Lowe and Harvey: Sialic acid in oral and maxillofacial malignancies. 1991; 49(8): 843-7.
- Raval GN, Parekh LJ, Patel DD, Jha FP, Sainger RN and Patel PS: Clinical usefulness of alterations in sialic acid, sialyltransferase and sialoproteins in breast cancer. Indian J Clin Biochem 2004; 19(2): 60-71.
- Mandal C and Mandal C: Sialic acid binding lectins. Experientia 1990; 46(5): 433–441.
- Sanjay PR, Hallikeri K, Shivashankara AR: Evaluation of salivary sialic acid, total protein and total sugar in oral cancer: A Preliminary report. Indian J Dent Res 2008; 19(4): 288-291.
- Fulcher CA: Metacycyclic chimeric pathway: Super pathway of sialic acid and CMP-sialic acid biosynthesis. Metacyc 2009.
- Warren L, Felsenfeld H: The Biosynthesis of sialic acids. The Journal of Biochemistry, 1962; 237(5): 1421-1431.
- Schauer R: Achievements and challenges of sialic acid research. Glycoconj J 2000; 17(7-9): 485-99.
- Narayanan S: Sialic acid as a tumor marker. Annals of Clinical and Laboratory Science 1990; 24(4): 376-384.
- The Cleveland clinic foundation, Department of Biochemistry, Cleveland, Ohio, USA. Serum sialic acid in normals and cancer patients, 1984; 22.
- Nair U, Oberl G and Nair J: Evaluation of frequency of micronucleated oral mucosa cells as a marker for genotoxic damage in chewers of betel quid with or without tobacco. Mutat Res 1991; 261: 163-68.
- Kayal JJ, Trivedi B, Nair J, Bhide V, Goswami C and Adhvaryu G. Incidence of micronuclei in oral mucosa of users of tobacco products singly or in various combinations. Mutagenesis 1993; 8: 31-3.
How to cite this article:
Madhumathi D: Level of sialic acid in oral cancer patients. Int J Life Sci & Rev 2015; 1(6): 207-10. doi: 10.13040/IJPSR.0975-8232.IJLSR.1(6).207-10.
All © 2015 are reserved by International Journal of Life Sciences and Review. This Journal licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 3.0 Unported License.
Article Information
1
207-210
579
1331
English
IJLSR
D. Madhumathi
Saveetha Dental College and Hospitals, 162, Poonamalle High Road, Velappanchavadi, Chennai, Tamil Nadu, India.
madhumathidevaraj@yahoo.com
13 May 2015
23 June 2015
28 June 2015
10.13040/IJPSR.0975-8232.IJLSR.1(6).207-10
30 June 2015